
ACUTE RENAL FAILURE AND ANCA ASSOCIATED VASCULITIS IN THE EDERLY.
Dra. Assumpta Serra.
Servei Nefrologia. Hospital Universitari Germans Trias i Pujol.
Badalona. Barcelona. Spain.
E-mail: 24177jbs@comb.es
| DISCUSSION BOARD |
The incidence of AAV is of 9-12 cases/million inhabitants year. In Spain the incidence is 7 cases/million inhabitants year. The first patients diagnosed with vasculitis were young or middle-aged, while nowadays, more cases are seen in the elderly. While in the eighties only 10% of the patients were over 65, in this decade, more than half of the patients have been older than 65. According to the Spanish Register of Glomerulonephritis data (1994-1999) (SRG), AAV is observed in 7% of all renal biopsies and in 18% of the biopsies in patients over 65 years of age.
Twenty-five per cent of the patients with AAV have precipitating events including infections, vaccines and previous history of drug taking (1). Twenty per cent of the patients have associated diseases with elderly patients having more associated diseases than younger patients, mainly diabetes mellitus, neoplasm and stroke (2).The presentation of MP is usually extrarenal (arthritis, respiratory tract involvement, skin lesions) or a combination of renal and extrarenal involvement. Isolated renal involvement is an uncommon presentation in MP, except in the elderly (2-3).The presentation of WG is usually extrarenal, always being extrarenal in CHSS, and always renal in RLV.
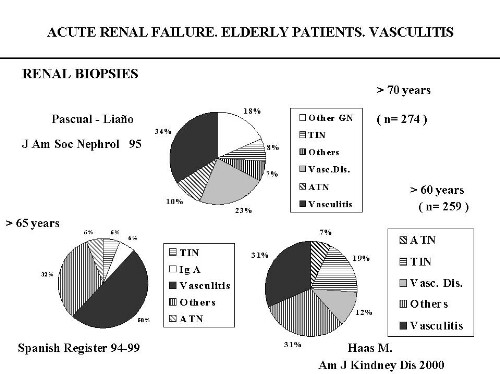
According to the SRG data, acute renal failure (ARF) is the most common form of renal presentation of AAV; ARF is more frequent as a mode of renal presentation in elderly patients than in young and middle-aged patients (64% versus 50%, respectively), and these patients more often present oliguria (30% versus 6%, respectively) (2,4). Vasculitis is also, the most common cause of ARF in the biopses of elderly patients (fig.1) with a prevalence from 31% to 50% of the cases (5-6)(SRG data).
After the kidney, lung and upper respiratory tract involvement are the most common organs affected in AAV. Organ involvement is similar in elderly and young patients. However, elderly patients with MP, have more arthritis and fewer lung infiltrates than younger patients and elderly patients with WG also have less upper respiratory tract involvement. This lack of clinical manifestations in the elderly may delay the diagnosis.
Renal biopsy (RB)is very useful in the diagnosis of AAV. Patients with ARF, should principally undergo biopsy when ARF is accompanied by microhematuria and/or proteinuria and/or positive ANCA. The presence of a positive ANCA titer aids in the diagnosis of the disease, but should not substitute RB, except when is contraindicated. RB is also useful in the selection of treatment and in achieving the renal prognosis of the disease.
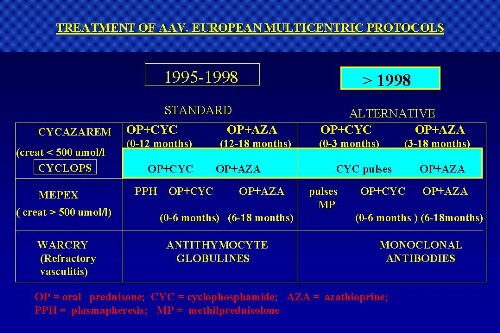
The objectives of treatment of vasculitis have changed over the years. Before 1988, the main aim was to increase patient and kidney survival. Since 1988, in addition to the previous objectives, others have appeared: to increase patient quality of life, decrease the side effects of treatment, reduce the incidence of relapse and provide dialysis and kidney transplant to these patients. Treatment of AAV is summarized in fig. 2 (7-8) with the data from several multicenter European protocols. If renal function is normal or slightly deteriorated, the standard treatment consists in oral prednisone (OP) and CYC. This treatment may be sustituted by OP and AZA in the remission phase of vasculitis (CYCAZAREM study results). The dosages of the different treatments are summarized in (7). Immunosuppressive drugs should be adjusted according to age and renal function (table I). Other possible therapies include the use of mycophenolate mofetil (9) and intravenous immunoglobulins (7).
|
DAILY ORAL PREDNISONE (OP)
DAILY ORAL CYCLOPHOSPHAMIDE (creatinine < 500 umol/l)
CYCLOPHOSPHAMIDE PULSES (every 2-3 weeks) (6-12 months)
|
The duration of treatment is not standarized with most groups recommending at least 18 months. In RLV patients who require dialysis, immunosuppressive drugs can be discontinued after 3 months. A balance must be maintained between the complications of treatment and disease remission (90% at 3 months with standard treatment). The main complications of treatment are: infection (24%-47%), neoplasm (2.5%-12%), diabetes mellitus (5-8%) and bone fractures (mainly in women above 65 years old). Elderly patients have the same percentage of infection as younger patients, but more severe (septicemia).
Some patients with vasculitis present one relapse of the disease, while others present several relapses (between 20% and 52% of the patients). The main organs involved in relapse are the skin, kidney and lung in MP, and the respiratory tract in WG. Relapse usually occurs when immunosuppressive treatment is decreased or withdrawn. Relapse may occur on dialysis and less frequently in transplanted patients. If vasculitis relapses, treatment should be restarted. Most centers use the ANCA titer to monitor treatment. Nevertheless, some patients may have high ANCA levels without vasculitis activity and, in contrast, a small proportion of patients may have active vasculitis with a negative ANCA titer.
The mortality rate of AAV patients is high with death mainly occurring during the first year of follow-up. Nevertheless, survival curves have improved in recent years (from 54% to 80% survival in the first year and from 38% to 80% survival in the fifth year ) (10). Elderly patients have worse survival curves than younger ones (1 year survival of 60%). Most deaths occur in the acute phase of the disease, usually within the first two years, mainly due to lack of response to treatment, septicemia (2-20% of deaths) or severe associated disease (hemorrhage, thrombosis, neoplasm, stroke). Long-term mortality is mainly due to relapse, side effects of treatment, and other causes (aging, heart disease). The following factors may contribute to bad prognosis of the disease: advanced aged, presence of associated diseases (commonly found in the elderly), creatinine levels at the time of presentation of vasculitis (>500 umol/l), and the presence of severe renal failure at the moment of presentation.
In conclusion, elderly patients with AAV have more acute renal failure, more associated renal disease, worse creatinine levels, more oliguria and less extrarenal clinical manifestations than younger patients at the time of presentation of vasculitis. Elderly patients have similar treatment complications than younger patients but more severe (septicemia, bone fractures), and lastly, elderly patients have worse survival curves than younger subjects.
REFERENCES
1. Serra A, Cameron JS. Vasculitis in the aged. In: Macias Nuñez JF, Cameron JS (eds). Renal function and disease in the elderly. London, Butterworths & Co.1987; 321-347.
2. Serra A, Martinez-Ocaña JC. Vasculitis con afectación renal predominante en pacientes mayores de 65 años. Nefrología 1997; 17 (supl. 3): 51-59.
3. Serra A, Cameron JS, Turner DR, Hartley B, Ogg CS, Neild GH, Williams DG, Taube D, Brown CB, Hicks JA. Vasculitis affecting the kidney: Presentation, histopathology and long-term outcome. Q J Med 1984; 53: 181-207.
4. Higgins RM, Goldsmith DJA, Connolly J, Scoble JE, Hendry BM, Ackrill P, Vening MC. Vasculitis and rapidly progressive glomerulonephritis in the elderly. Postgrad Med J 1996; 72: 41-44.
5. Haas M, Spargo BH, Wit EJ, Meehan SM. Etiologies and outcome of acute renal insufficiency in older adults: a renal biopsy study of 259 cases. Am J Kidney Dis 2000; 35: 433-447.
6. Pascual J, Liaño F, Ortuño J. The elderly patient with acute renal failure. J Am Soc Nephrol 1995; 6: 144-153.
7. Jayne DRW, Rasmussen N, For the European Community Systemic Vasculitis Clinical Trials Study Group (ECSYSVASTRIAL). Mayo Clin Proc 1997; 72: 737-747.
8. Haubitz M, Schellong S, Göbel U, Schurek HJ, Schaumann D, Koch KM, Brunkhorst R. Intravenous pulse administration of cyclophosphamide versus daily oral treatment in patients with antineutrophil cytoplasmic antibody-associated vasculitis and renal involvement. Arthritis & Rheumatism 1998; 41: 1835-1844.
9. Nowack R, Göbel U, Klooker P, Hergesell O, Andrassy K, van der Woude FJ. Mycophenolate Mofetil for maintenance therapy of Wegener´s granulomatosis and microscopic polyangiitis: A pilot study in 11 patients with renal involvement. J Am Soc Nephrol 1999; 10: 1965-1971.
10. Fuiano G, Cameron JS, Raftery M, Hartley JR, Williams DG, Ogg GS. Improved prognosis of renal microscopic polyarteritis in recent years. Nephrol Dial Trasplant 1988; 3: 383-391.