
Peritoneal dialysis access - is it time
to move up?
Professor Emeritus of Medicine
E-mail: Twardowskiz@health.missouri.eduZbylut J. Twardowski, MD, PhD, FACP
Division of Nephrology, Department of Medicine, University of Missouri
Columbia, Missouri, USA
| DISCUSSION BOARD |
INTRODUCTION
Traditionally, peritoneal catheters have been implanted through the abdominal wall with the exit in the abdominal integument; however, there are theoretical arguments and clinical experiences indicating that moving the exit up to the chest decrease catheter related complications and improves its survival probability. Such a catheter was designed in 1991 and has been manufactured since that time. The tenth anniversary of clinical experience with this catheter passed last August.
Design
The presternal peritoneal dialysis catheter is composed of two flexible (silicon rubber) tubes, which are connected end to end at the time of implantation (Figure 1). The implanted abdominal tube constitutes the intraperitoneal catheter segment and a part of the intramural segment. The distal end of the abdominal tube, located in the peritoneal cavity, is coiled and contains the central bore with multiple small side perforations provided for fluid delivery into and drainage from the peritoneal cavity. The proximal end of the abdominal tube carries a polyester cuff, to be located in the rectus muscle (Figure 1. The tubing is also provided with a flange circumferentially surrounding the tubing just below the cuff and a bead adjacent to the flange. As in the swan neck Missouri catheter the flange and bead are slanted at an angle of about 45o. After implantation, the proximal end of the abdominal tube extends a few centimeters from the cuff and is provided with a connector made of titanium (Figure 1). The connector is to be coupled with the distal part of the thoracic part at the time of implantation. The thoracic tube constitutes the remaining part of the intramural segment and the external catheter segment. The distal end bore of the thoracic tube communicates with the proximal end bore of the abdominal tube through the titanium connector. The tube carries two porous cuffs (Figure 1), a superficial cuff and a middle or central cuff. The tube between the cuffs has a permanently bent section (swan neck feature) defining an arc angle of 180o (Figure 1). Both tubes have a radiopaque barium stripe, which helps achieve proper alignment of the tubes during implantation. The stripe is also useful during insertion and post-implantation care, facilitating recognition of catheter twisting. The proximal tube is trimmed to the desired length during implantation.

Catheter implantation technique
A detailed implantation technique is described a in a book chapter [1] and a video [2]. Here only general principles of implantation are given. Patient preparation before catheter implantation is very important. The tunnel is marked by a nurse taking into consideration the presence of previous scars, right or left-handedness, and the patient's preference.
On the chest, a superficial cuff is marked at the second or third intercostal space and the exit 2 - 3 cm from the cuff in the presternal or parasternal area. It is preferable not to cross the midline in patients likely to have heart surgery. One gram of Vancomycin is given by slow intravenous infusion within 24 hours prior to surgery. Cephalosporins (1.0 g IV 1 hr preoperatively repeated 12 hr postoperatively) also constitute appropriate prophylactic therapy [3].
The surgical technique of catheter implantation used for "swan neck" catheters is generally followed with modifications unique to the new design. The intraperitoneal segment, bead, flange, and deep cuff are implanted identically to that of swan neck Missouri catheters. Stripe must face the front. A purse string suture is tied between the flange and the bead. For implantation of the upper segment, a vertical 3-4 cm incision is made parasternally at the level of the second and third ribs. Two small subcutaneous pockets are made one on each side of the incision to accommodate the bent section of the upper (chest) tube of the catheter. The pockets are dissected enough to accommodate the middle and superficial cuffs. To join the upper and lower tube, a tunneling device is pushed from the abdominal to the sternal incision. The abdominal end of the upper tube is grasped with the spring clamp and pulled caudally through the sheath, and the tunneling device is removed by pulling in the caudal direction.
The middle cuff of the upper tube is carefully placed in the subcutaneous pocket. When the catheter is appropriately positioned, the desired lengths of the tubes are measured and the tubes are trimmed. The titanium connector is secured with sutures placed over the connector grooves on both the abdominal and thoracic tubes. The stripes on both tubes are facing forward. Both sutures are tied together (Figure 2) and the titanium connector is positioned in the subcutaneous tissue approximately 2 - 6 cm above the rectus sheath incision. After the connection is made, a trocar of the same size as the catheter tubing is attached and carefully passed through the pocket and the external exit indicated by the stencil mark. The wounds are checked for leaks, irrigated, inspected for hemostasis, and closed with sutures.

Catheter removal
Removal of a swan neck presternal peritoneal dialysis catheter is a surgical procedure performed in the operating room. The procedure has been previously described [1].
Long term results.
Since August 1991, at the Division of Nephrology, Department of Medicine, University of Missouri, all patients without contraindications to peritoneal catheter implantation and commencing peritoneal dialysis or requiring catheter replacement were offered a choice of a presternal or an abdominal catheter. Patients with relative contraindications to abdominal catheters, such as extreme obesity and abdominal ostomies, were encouraged to choose presternal catheter.
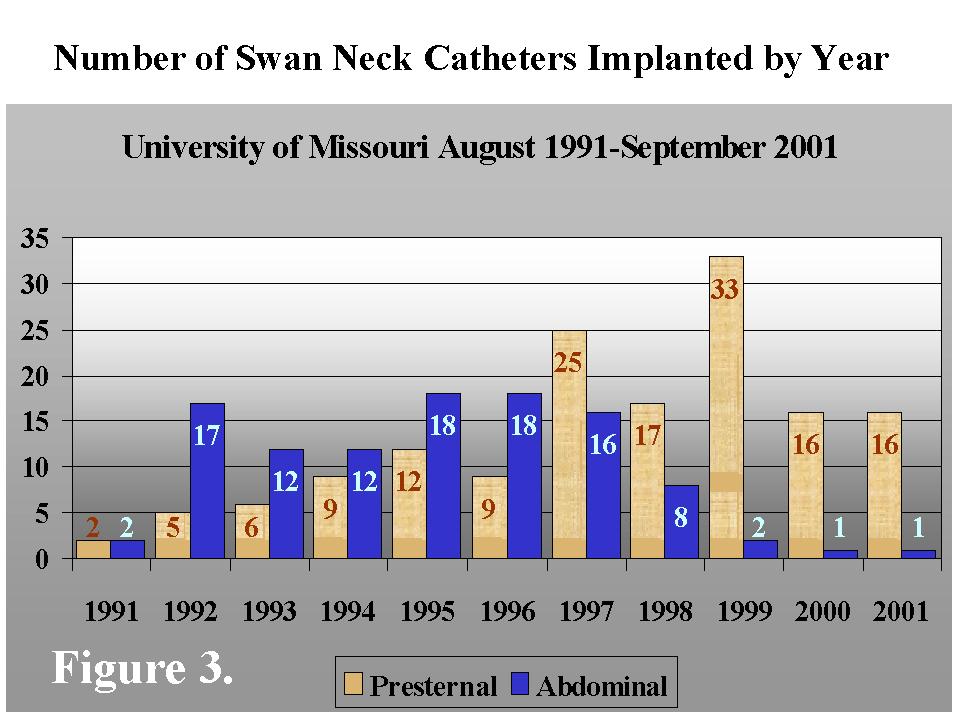
Four-year [4] and six-year [5] experiences with presternal catheters have been already published. This last paper reported data on 58 catheters inserted from August 1991 to October 1997. The overall experience was 61 patient-years. Presternal catheter survival probabilities (95% at two years and 86% at three years) were excellent; exit, tunnel infections, and other complications tended to be lower compared to abdominal catheters. Catheters failed only because of refractory/recurrent peritonitis. Since that report, 92 additional presternal catheters have been implanted. As shown in Figure 3 from August 1991 to September 2001, 150 of presternal catheters and 98 abdominal catheters were implanted at the University of Missouri. Most of the catheters (109) were implanted in patients followed at the Dialysis Clinic, Inc., in Columbia, but 41 were implanted for other clinics in Missouri. Gradually, swan neck presternal catheters became more popular among the patients followed by the Division of Nephrology, Department of Medicine, University of Missouri. The longest survival of the presternal catheter as of October 2001 is 7.9 years, and the catheter is still functioning. As reported previously [5], open-heart surgeries were performed in three patients with presternal catheters without damaging the catheters. This was possible due to the parasternal placement of the chest part, on the same side as the abdominal part. As the catheters did not cross the midline they did not interfere with the sternal incision. These catheters were used the next day after surgery for peritoneal dialysis. We found it valuable to discuss the details of the catheter location with a thoracic surgeon before heart surgery.
The overall experience with the presternal catheters gathered in over 130 patient-years indicates that these catheters are particularly useful in obese patients (BMI > 35), patients with ostomies, and patients who want to enjoy tub bathing without a risk of exit contamination due to submersion in stagnant water. Contrary to poor experience with cuff shaving in abdominal catheters [6] and similar to the experience of Piraino et al [7], our experience with cuff shaving in presternal catheters proved to be very successful, probably due the presence of three cuffs and a long tunnel. In presternal catheters the abdominal and thoracic segments may be replaced separately, which permits uninterrupted ambulatory peritoneal dialysis if only the thoracic segment is exchanged.
Main indications for presternal catheters in children were: recurrent exit site infections with abdominal catheters, the presence of ureterocutaneostomies, obesity, the use of diapers, young age, and fecal incontinence [8]. Exit site infection rates as low as 1/162 patient-months have been reported in children with presternal catheters [9].
Disadvantages of the presternal catheter are few. Because of longer tubing, presternal catheter drain flow rates are slower than abdominal catheters [10], but none of the patients complained about the drain time and neither patients nor peritoneal dialysis nurses who had experience with both types of catheters noticed the difference prior to the timing study. Another complication related to the length of the catheter and the presence of the additional titanium connector is a possibility of bacterial colonization of the catheter/connector related to peritonitis. Two such occurrences were previously reported [4].
In our series, one catheter disconnected within the tunnel, but the leak was easily diagnosed and the catheter repaired without interrupting ambulatory peritoneal dialysis. This complication is more frequent in children as they grow after catheter implantation. In spite of leaving an extra catheter length in the subcutaneous tunnel at the time of implantation, this complication was noted in 2 of 11 catheters, 7 and 33 months after implantation [9]. Finally, the implantation of the catheter is technically difficult; therefore, in spite of excellent results, its use is spreading rather slowly and only in centers with excellent surgical service.
Because of difficulties in implantation and risk of disconnection within the tunnel of the two parts secondary to rapid children growth in the first year of life, Chadha et al. [11] used a conventional swan neck catheter, but larger than typically required, placed with its exit site located on the chest wall. The results of this approach in small infants with colostomy were excellent.
Comment
Low exit and tunnel infection rates and peritonitis episodes with presternal catheters are related to the specific catheter design and the exit in the chest. A major cause of exit site infection is trauma at the site where the superficial cuff binds with the surrounding tissue. This may be caused by pulling on the catheter, twisting, pressure on the exit by a tight garment, or movement of the patient's abdominal wall transmitting mechanical stress to the exit [12]. Avoidance of mechanical stress and good immobilization are extremely important for good healing and prevention of exit site infection, especially during break-in [13]; however, all efforts to immobilize the abdominal catheter with use of various devices have been only partially successful because the abdomen is very mobile. Any change of the body position results in abdominal wall motion. This motion is transmitted to the catheter, causes piston like movement within the sinus tract, traumatizes the exit and sinus, and brings about bacterial penetration deep into the sinus. Damage to the epidermis and/or granulation tissue within the sinus combined with the deep bacterial penetration results in infection.
Clinical surgical experience indicates that wounds heal better after thoracic surgery than after abdominal surgery; this may be related to less chest mobility or some other reasons. The chest is a very sturdy structure, with minimal wall motions, especially of the upper chest and over the sternum, compared to the abdominal wall. The catheter exit located over the sternum is subjected to only minimal movement. Decreased piston-like movement of the catheter within the sinus reduces inward conveyance of outer sinus tract flora. Moreover, a tight garment is usually not worn on the chest and there is less pressure on the exit.
In peritoneal dialysis patients with abdominal ostomies, the chest location of the catheter exit, away from the ostomies, reduces the risk of exit contamination. Obese patients have higher exit site infection rates [14] and a tendency to poor wound healing, particularly after abdominal surgery. The subcutaneous fat layer is several times thinner on the chest than on the abdomen. If fat thickness per se is responsible for quality of healing and susceptibility to infection, then the chest location may be preferred for obese patients. All these favorable factors may significantly reduce exit site infections. The chest location of the exit is particularly advantageous in small children because of the greater distance from diapers. A long catheter tunnel combined with three cuffs, curtails pericatheter bacterial penetration into the peritoneal cavity, thus reducing incidence of peritonitis
The presternal catheter is also advantageous for psychosocial reasons. Many patients prefer to have a catheter on the chest because of body image; however, others may prefer the catheter exit on the abdomen. A chest exit location allows a deep tub bath without the risk of exit contamination. The patients who prefer a tub bath to a shower favor the presternal catheter. Some patients choose the presternal catheter because of the easier exit site care using a magnifying mirror. The majority of patients at the University of Missouri choose the presternal catheter for psychosocial reasons.
Except for the body image concerns for some patients, disadvantages of the presternal catheter are minimal. Dialysis solution flow is slowed down a little due to the increased catheter length; however, this increase constitutes only a fraction of the overall time of inflow and outflow, and the slower flow is insignificant clinically. There is a possibility of catheter disconnection in the tunnel but this complication is extremely rare in adults. It is more frequent in children because the intra-tunnel segment is stretched as they grow. Finally, the implantation technique is more difficult compared to that of single piece, abdominal catheters. Because of the catheter length and the presence of another titanium connector the catheter may become colonized during an episode of peritonitis with consequent recurrent peritonitis episodes.
In conclusion, experience with presternal peritoneal dialysis catheter documents patient acceptance, fewer complications, and improved outcomes. It is time to "move up" the catheter exit site to the chest wall.
1. Twardowski ZJ, Nichols WK: Peritoneal dialysis access and exit site care including surgical aspects. In: Peritoneal Dialysis. Edited by Gokal R, Khanna R, Krediet RT, Nolph KD. Kluwer Academic Publishers, Dordrecht/Boston/London, Second Edition, 2000 (Chapter 9): 307 - 361.
2. Twardowski ZJ, Nichols WK, Khanna R, Nolph KD. Swan neck presternal peritoneal dialysis catheter: design, insertion, and break-in. Video produced by the Academic Support Center, University of Missouri, Columbia, MO, U.S.A., 1993, available through Kendall Healthcare, 15 Hampshire Street, Mansfield, Massachusetts 02048, USA, the manufacturer and distributor of swan neck catheters.
3. Gokal R, Alexander S, Ash S, Chen TW, Danielson A, Holmes C, Joffe P, Moncrief J, Nichols K, Piraino B, Prowant B, Slingeneyer A, Stegmayr B, Twardowski Z, Vas S: Peritoneal catheters and exit-site practices toward optimum peritoneal access: 1998 update (Official report from the International Society for Peritoneal Dialysis). Perit Dial Int 1998; 18 (1): 11-33.
4. Twardowski ZJ, Prowant BF, Pickett B, Nichols WK, Nolph KD, Khanna R: Four-year experience with swan neck presternal peritoneal dialysis catheter. Am J Kidney Dis 1996; 27 (1): 99 -105.
5. Twardowski ZJ, Prowant BF, Nichols WK, Nolph KD, Khanna R: Six-year experience with swan neck presternal peritoneal dialysis catheter. Perit Dial Int 1998; 18 (6): 598-602.
6. Twardowski ZJ, Prowant BF. Exit site study methods and results. Perit Dial Int 1996; 16 (Suppl 3): S6-S31.
7. Piraino B, Bernardini J, Peitzman A, Sorkin M. Failure of peritoneal catheter cuff shaving to eradicate infection. Perit Dial Bull 1987; 7:179-182.
8. Sieniawska M, Roszkowska-Blaim M, Warchol S. Swan neck presternal catheter for continuous ambulatory peritoneal dialysis in children. Pediatr Nephrol. 1993 Oct;7(5):557-8.
9. Warchol S, Roszkowska-Blaim M, Sieniawska M Swan neck presternal peritoneal dialysis catheter: five-year experience in children. Perit Dial Int. 1998 Mar-Apr;18(2):183-7.
10. Prowant B, Ponferrada L. Clinical drain flow rates of Tenckhoff and swan-neck catheters. Perit Dial Int 1998; 18:(suppl 1), S39.
11. Chadha V, Jones LL, Ramirez ZD, Warady BA. Chest wall peritoneal dialysis catheter placement in infants with a colostomy. Adv Perit Dial. 2000;16:318-20.
12. Twardowski ZJ, Prowant BF: Can new catheter design eliminate exit site and tunnel infections? Perspectives in Peritoneal Dialysis. 1986; 4 (No. 2): 5 - 9.]
13. Twardowski ZJ, Prowant BF: Exit-site healing post catheter implantation. Perit Dial Int 1996; 16 (Suppl 3): S51-S70.
14. Kim D, Burke D, Izatt S, Mathews R, Wu G, Khanna R, Vas S, Oreopoulos G: Single or double cuff peritoneal catheters? A prospective comparison. Trans Am Soc Artif Intern Organs. 1984; 30: 232 - 235.
REFERENCES
Corresponding author:
Zbylut J. Twardowski M.D.
Dialysis Clinic, Inc
3300 LeMone Industrial Blvd. Columbia, MO 65201, U.S.A.
E-mail: Twardowskiz@health.missouri.edu