|
Paneles de Discussión
Paneais de Discussio Comunicaciones libres
Comunicaçoes livres |
CARNITINE SUPPLEMENTATION IN HEMODIALYSIS PATIENTSCharles Chazot, M.DCentre de Rein Artificiel, Tassin, Francechchazot@club-internet.fr1- What is carnitine?. Carnitine metabolism has been recently reviewed [1]. Carnitine is a 161 dalton water-soluble compound discovered in 1905 from muscle tissue, explaining the name given to this molecule. It was shown to be the mandatory growth factor for a flour worm, Tenebrio Molitor and called vitamin BT. In 1955 were demonstrated the reversible acetylation of the molecule and its involvement in fatty acid metabolism. Carnitine is necessary for long chain fatty acids to enter mitochondria and to undergo b-oxydation. It also shuttles acyl- and acetyl-residues in and out of mitochondria. Carnitine sources are mainly meat and dairy products and represent 75% of carnitine supply (40-70 mg/day). Intestinal transport of carnitine is active, but also passive when the ingested amount is high. Endogenous synthesis is possible in the liver and kidney from lysine and methionine, requiring vitamins C and B6. 6-N-Trimethyllysine residues produced from proteolysis are used for endogenous carnitine synthesis. In the tissues, carnitine pool is mainly distributed in skeletal muscle that represents 98% of the pool. A small amount is found in the liver. The usual reported plasma concentrations of carnitine are 35-65 µmoles/l for total carnitine totale, 30-55µmoles/l for free carnitine with a ratio acy/free carnitine lt; 40%. Carnitine is filtered at the glomerulus and 100-300 µmoles/ day are excreted in the urine, mainly as acyL-carnitine residues.
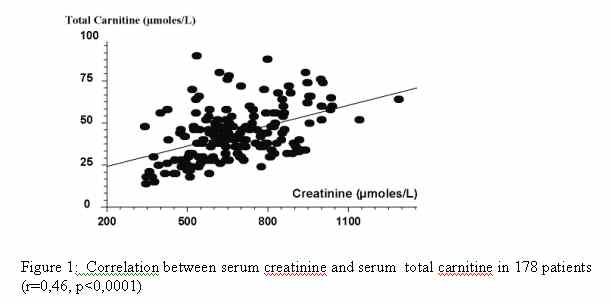
2- Carnitine in hemodialysis patients. In dialysis patients, carnitine handling has been studied extensively [2]. It is freely permeable across the dialysis membrane and losses occur during dialysis treatment. A 27-68% reduction of plasma carnitine between pre- and post-dialysis values has been reported. The amount excreted in dialysate has been measured at 190-2100 µmoles/session. Data on the total and free plasma or serum carnitine concentrations in hemodialysis (HD) patients have been conflicting [3]. However, carnitine deficiency is often reported in this setting. In a large cohort of 178 patients, we found that 49% of patients had plasma free carnitine below the minimal range, with 47% of patients with a acyl/free carnitine ratio over 0,4 [4]. We found that plasma total carnitine was correlated with serum creatinine (Figure 1) and protein intake, but not with C-reactive protein level. Then plasma carnitine concentration may be used as a nutritional marker. Time spent on dialysis contribute to decrease of plasma carnitine levels [5] and also carnitine concentration in muscle [6]. Also, carnitine content of muscle has been found correlated with peak exercise time by the same author. Recently, Constantin-Teodosiu found that free carnitine in plasma was correlated negatively with age and positively with hand-grip strength only in female but not in male patients [7].
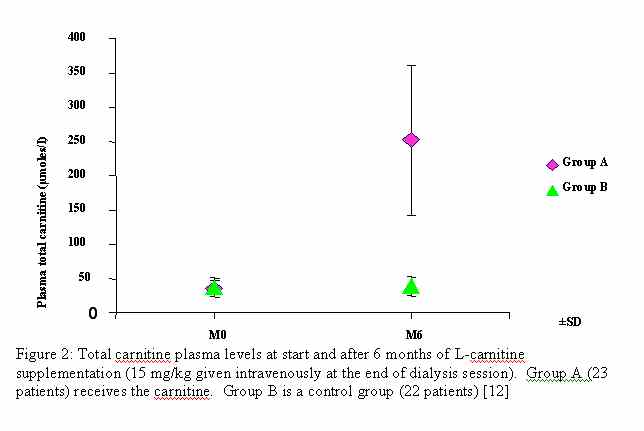
3-Carnitine provision in hemodialysis patients. Evidence-base data. Carnitine has been given to hemodialysis patients for the first time in 1978 by Bizzi et al [8]. Since that time, many trials have used exogenous carnitine administration for several purpose including anemia, cramps and muscle symptoms, dyslipidemia, quality of life and cardiac failure. Route and dose of carnitine administration to dialysis patients has been recently reviewed by Evans [5]. Only L-carnitine form is usable for therapy in human beings, the DL racemic molecule being toxic [9]. Oral route has been used to supplement dialysis patients. Bioavailability (low -15%- in healthy subjects) is unknown in this condition. Oral carnitine is a source of trimethylamine (a fishy-odor compound) and trimethylamine-N-oxide that accumulate in uremia with unknown potential toxicity [5]. Intravenous route is widely used in most of the clinical supplementation studies in hemodialysis patients at a usual dose of 20 mg/kg at the end of each hemodialysis treatment during several months. Plasma carnitine increases dramatically after several injections, reaching supra-physiological levels (Figure 2). Muscle carnitine concentrations increase by 60-200% after 6 weeks of treatment. No toxicity has yet been reported with these high levels. The two major contributions studying clinical effects of carnitine supplementation in dialysis patients are the meta-analysis by Hurot et al [10] and the DOQI guidelines for nutrition [11]. In their meta-analysis, Hurot et al [10] reviewed 83 studies whose twenty-one were randomized. Eighteen studies were used including 482 patients for the meta-analysis. Carnitine supplementation is inefficient to improve lipid profile on triglycerides, total cholesterol, and HDL, LDL, VLDL fractions. It improves anemia and decrease EPO consumption. For methological reasons, the meta-analysis was unable to conclude for a beneficial effect of L-carnitine supplementation on myocardial function, arrhythmia, asthenia and fatigue, exercise capacity and muscle weakness. The guideline #22 from K-DOQI nutrition [11] does not recommend routine provision of carnitine because of lack of evidence. However, it is added that anemia treatment is the most promising field for supplemental carnitine therapy in dialysis patients.
4- National Kidney Foundation. The Carnitine Consensus Conference. The 2003 April issue of the American Journal of Kidney Disease includes an article entitled "Practice Recommendations for the use of L-carnitine in hemodialysis patients" [14]. These recommendations have been issued during the Carnitine Consensus Conference from a panel of experts, in the name of the National Kidney Foundation. A supplement is associated with this AJKD issue, entitled "The role of L-carnitine therapy in patients on hemodialysis". including several reviews of carnitine disorders and effects. First, a "dialysis-related carnitine disorder" (DCD) syndrome is defined. This syndrome includes anemia (inability to reach or maintain haemoglobin target or hyporesponse to EPO), intradialytic hypotensions, cardiomyopathy and muscle weakness and fatigability affecting quality of life. Second, carnitine assessment is not required to diagnose CDC because no relationships have been established between plasma carnitine levels and the severity of symptoms. However, normal plasma free carnitine levels and acyl/free carnitine ratio exclude DCD. Third, recommendations are given to prescribe to these patients 20 mg/kg of intravenous L-carnitine three times a week for 9 to 12 months, with evaluation at three months intervals. Several comments arise from these recommendations.
5- Conclusions. Carnitine supplementation in dialysis patients remains an unsolved issue, whereas carnitine deficiency in plasma and tissues (skeletal muscle) is obvious in many patients after several years on hemodialysis treatment. The absence of effects on lipids abnormalities is now documented. It seems reasonable to use L-carnitine to improve EPO response (and to decrease EPO dose) even if this hot topic deserve complementary studies. For the other fields like intradialytic hypotension episodes, chronic hypotension, myocardiopathy, muscle weakness, cramps, nutrition, quality of life, correctly designed studies are necessary to evaluate the clinical benefits before L-carnitine administration is routinely prescribed on a large scale to dialysis patients for these conditions relying on multifactorial disorders.
REFERENCES
1. Hoppel C: The role of carnitine in normal and altered fatty acid metabolism. Am J Kidney Dis 41:S4-S12., 2003
2. Bohmer T, Bergrem H, Eiklid K: Carnitine deficiency induced during intermittent haemodialysis for renal failure. Lancet 1:126-128., 1978
3. Ahmad S: L-carnitine in dialysis patients. Semin Dial 14:209-217., 2001
4. Chazot C, Jean G, Vo Van C, Charra B, Terrat JC, G. L: Serum carnitine as a marker of protein malnutrition (Abstract). J Am Soc Nephrol 8:230A, 1997
5. Evans A: Dialysis-related carnitine disorder and levocarnitine pharmacology. Am J Kidney Dis 41:S13-26., 2003
6. Hiatt WR, Koziol BJ, Shapiro JI, Brass EP: Carnitine metabolism during exercise in patients on chronic hemodialysis. Kidney Int 41:1613-1619., 1992
7. Constantin-Teodosiu D, Young S, Wellock F, Short AH, Burden RP, Morgan AG, Greenhaff PL: Gender and age differences in plasma carnitine, muscle strength, and exercise tolerance in haemodialysis patients. Nephrol Dial Transplant 17:1808-1813., 2002
8. Bizzi A, Mingardi G, Codegoni AM, Mecca G, Garattini S: Accelerated recovery of post-dialysis plasma carnitine fall by oral carnitine. Biomedicine 29:183-184., 1978
9. Bazzato G, Mezzina C, Ciman M, Guarnieri G: Myasthenia-like syndrome associated with carnitine in patients on long-term haemodialysis. Lancet 1:1041-1042., 1979
10. Hurot JM, Cucherat M, Haugh M, Fouque D: Effects of L-carnitine supplementation in maintenance hemodialysis patients: a systematic review. J Am Soc Nephrol 13:708-714., 2002
11. Clinical practice guidelines for nutrition in chronic renal failure. K/DOQI, National Kidney Foundation. Am J Kidney Dis 35:S1-140., 2000
12. Chazot C, Blanc C, Hurot JM, Charra B, Jean G, Laurent G: Nutritional effects of carnitine supplementation in hemodialysis patients. Clin Nephrol 59:24-30., 2003
13. Ahmad S, Robertson HT, Golper TA, Wolfson M, Kurtin P, Katz LA, Hirschberg R, Nicora R, Ashbrook DW, Kopple JD: Multicenter trial of L-carnitine in maintenance hemodialysis patients. II. Clinical and biochemical effects. Kidney Int 38:912-918., 1990
14. Eknoyan G, Latos DL, Lindberg J: Practice recommendations for the use of L-Carnitine in dialysis-related carnitine disorder National Kidney Foundation Carnitine Consensus Conference. Am J Kidney Dis 41:868-876., 2003
15. Pauly DF, Pepine CJ: The role of carnitine in myocardial dysfunction. Am J Kidney Dis 41:S35-43., 2003
16. Casciani C, Caruso U, Cravotto E, Corsi M, Maccri F: Beneficial effects of L-carnitine in post-dialysis syndrome. Curr Ther Res 32:116-127, 1982
17. Steinman TI, Nissenson AR, Glassock RJ, Dickmeyer J, Mattern WD, Parker TF, 3rd, Hull AR: L-carnitine use in dialysis patients: is national coverage for supplementation justified? What were CMS regulators thinking--or were they? Nephrol News Issues 17:28-30, 32-24, 36 passim., 2003
18. Bohmer T, Rydning A, Solberg HE: Carnitine levels in human serum in health and disease. Clin Chim Acta 57:55-61., 1974 |