|
Paneles de Discussión
Paneais de Discussio Comunicaciones libres
Comunicaçoes livres |
MORPHOLOGIC DIAGNOSIS OF CRESCENTIC GLOMERULOPATHIES. (CRESCENTIC GLOMERULITIS OR CRGL) Dr. Ernesto O. Hoffmann. Professor of Pathology. Louisiana State University Medical Center and VA Medical Center. New Orleans, Louisiana, USA. ehoffm@lsuhsc.edu Introduction
Glomerular crescents (CRs), necrosis, endothelio mesangial cell proliferation, inflammation and more remotely thrombosis and mesangial cell proliferation are usually complications closely associated and usually superimposed on other glomerulopathies (GPs). These lesions may be focal or diffuse, segmental or global. The same disease may some times have only one of the lesions mentioned. Some other times it may have all those lesions in the same renal biopsy. For didactic reasons, tradition and because there are truly predominating patterns, we have sub divided this group of complications in five morphologic patterns:
2. Thrombotic Microangiopathic Glomerulitis (TMGL). These two patterns are easier to identify in the renal biopsy and are discussed elsewhere6). 3. Crescentic GL (CRGL). Here the predominating lesion in the biopsy are crescents. This is the pattern discussed in this page. 4. Vasculitic Glomerulitis (VAGL). Here vasculitis predominates in the biopsy. 5. Necrotizing Glomerulitis (NEGL). Necrosis is the predominating lesion. It is obvious that overlapping of these patterns (complications) is frequently seen in renal biopsies and clinical information becomes crucial for the differential diagnosis of disease. In this conference I am presenting a different approach for the morphologic diagnosis and classification of GP with CRs (group 3 above or CRGL). Similar morphologic classification of CRGPs is available in the literature5. CRESCENTIC GLOMERULITIS (CRGL).
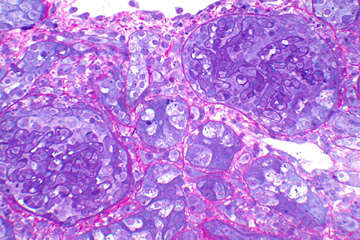
b. A complication superimposed on another GP [Post infectious GN, Systemic Lupus Erithematosus (SLE), Alport's Syndrome, Fabry's disease, other]5; c. Associated to other conditions (leukemia, sepsis, renal infarct); d. Idiopathic or of unknown cause. Has no evidence of associated NP, extra glomerular or extra renal disease]. CRs are found in many seemingly diverse conditions and are important because they are signs of severe activity and poor prognosis. Sometimes CRs are inconspicuous (thrombotic micro angiopathies, periphery of infarcts, metabolic diseases). Some other times they are the most prominent feature of the GP (SLE, Anti-GBM GN, post-infectious GN, Henoch Schonlein GP, vasculitis). CR are usually associated with necrosis, fibrin deposition, cell proliferation, inflammation, thrombosis, sclerosis, fibrosis, and alteration of the capillary tufts. CRs may show different "ages": epithelial, fibro epithelial and fibrous (Illustrations 1). Illustrations 1
BASIC MORPHOLOGY AND AGE OF THE CRESCENTS
Most authors agree that any GP may show crescents. However, Crescentic Glomerulonephritis (Glomerulopathy) (CRGP) is a term applied to glomerulopathies that share the common lesion of CRs in a "large percentage of glomeruli". However, there is no agreement on the % of glomeruli involved with CR [20%13. 30%5. 50%9, 10. 80%13] to call a GP CRGP. CRGP is also called Rapidly Progressive GN but, it is also stated that "CRGP" is not synonymous of rapidly progressive GN since less than 50% of the crescentic glomerulopathies have clinical rapidly progressive NP5. The reverse is probably also true. There is a large group of CRGP called "Idiopathic or Primary Crescentic GP", this group is divided in three subgroups9,10: 1. Anti GBM CRGP (or Goodpasture Syndrome). If the cause is known (anti GBM ab) it can not be called Idiopathic. It is not Primary either since it may not be restricted to the kidney (Goodpasture syndrome). 2. CRGP with underlying immune complex GP. (Caused by immune complexes, also idiopathic??. Also includes processes not restricted to the kidney (Henoch-Schonlein GN, SLE GN)] therefore, also not Primary. 3. CRGPs without immune complexes or anti GBM antibodies or "Pauci-immune" CRGP. Anti neutrophil cytoplasmic antibodies test (ANCA)3 is said to be a marker for the latter group 3. However, ANCA positive tests have also been reported in anti-GBM GN, immune complex GN, other GP and in extra-renal diseases7. ANCA positivity alone, in the absence of appropriate pathologic findings, should not be used to substantiate a morphologic diagnosis of vasculitis (Wegener's or Micro Polyarteriris nodosa)4, 12. "ANCA Associated GN" is not a morphologic term therefore, I suggest not to be used as a morphologic diagnosis. The search for "Crescentic glomerulonephritis" in the Internet yields a large number of pauci-immune GPs with CRs that have no association with vasculitis therefore, that term is erroneously used to single out ANCA positive GPs. Crescentic glomerulopathies are apparently a very rich soil for the "fabrication of new diseases". When the pathologist is confronted with the renal biopsy and finds a GP with CRs, some of the previous definitions and concepts are of no help and frequently they are very confusing. I believe that it is easier and less problematic for the Pathologist to make a morphologic diagnosis according to what he sees in the renal biopsy, regardless of the clinical nomenclature, ANCA tests, definitions and other controversial concepts published in the literature. Reading the renal biopsy by the pathologist: The sample is adequate: The first step in examining a renal biopsy is to determine if the sample is adequate. Most renal GPs have focal or focally accentuated lesions. If only 10% of the glomeruli in the kidneys are involved by a focal process, a biopsy sample with ten glomeruli has a 35% probability of missing the diagnostic lesions. When 25% of the glomeruli are involved it is still a 5% chance of missing the diagnostic lesions2, 15. The number of glomeruli in the biopsy is even more crucial for the assessment of the grade (activity) and stage (chronicity) of the process. Hence, a biopsy with at least 20 to 25 glomeruli is sufficient for this purpose2, 15. The report of the pathologist must include the # of glomeruli in the biopsy to give the clinician an idea on how accurate the pathologists report may be according the size of the biopsy.
Illustrations 2
MORPHOLOGIC DIAGNOSIS OF CRESCENTIC GLOMERULOPATHIES.
1. The renal biopsy has CRs and underlying GP (Illustrations 2):
1.2. GP with metabolic or other non-immune deposits (GO); 1.3. GP with derangement of the anatomic components of the glomeruli (GD); 1.4. Other glomerulitis or complications (GL). Report the GP with the current name and % of crescents, age and necrosis. Examples: Post Infectious GN with 45% fibro epithelial crescents, 10% with necrosis; Alport's Glomerulopathy with 10% epithelial crescents and no necrosis; Thrombotic microangiopathy with 5% epithelial crescents and no necrosis. The best glomeruli to identify the underlying GP are those without CRs. The CRGP has no underlying GP or due to the collapse and destruction of the glomerular tufts, the underlying GP can not be recognized, see if it fits into one of the groups below. 2. The renal biopsy has CRs but no recognizable underlying GP. TEM, HRLM and FM are negative for immune deposits. FM shows linear pattern with C3 and IgG along the GBM (Illustrations 2):
3. The renal biopsy shows glomerular CRs but no recognizable underlying GP. FM, HRLM and TEM are negative for Immune deposits. No linear pattern by immunohistology (Illustrations 2).
3.1. Biopsy positive for vasculitis: Report type of vasculitis and % of CRs and necrosis. Example: Micro Polyarteritis Nodosa with 40% crescents. 10% epithelial crescents with necrosis, 20% fibro epithelial crescents without necrosis, 10% fibrous crescents without necrosis. History of positive P-ANCA. Positive C-ANCA, presence of granulomata (Glomerular or extra glomerular) or periglomerulitis with rupture of the capsule of Bowman, are suggestive but not pathognomonic of Wegener's GP. However, do not use ANCA results to classify morphologically CRGPs. 3.2. Biopsy negative for vasculitis:
3.2.2. Positive history of Leukemia, infections, infarct (ANCA??). Report: CRGL with % CRs, % necrosis and age. History of, or associated to, or consistent with: Leukemia, renal infarct, infections, other. 4. No underlying GPs, FM negative, HRLM and TEM are non contributory, no vasculitis, no sepsis, no medication toxicity, no renal infarct (ANCA??). (Illustrations 2). Report: Idiopathic GP with 40% crescents (30% fibro epithelial, 10 % fibrous). No necrosis. A large number of biopsies with CRs may end up in this latter group. Due to the collapse and destruction of the glomerular tufts, the underlying GP can not be recognized and/or there is no clinical history available. This is a true "idiopathic" group, the cause is unknown5.
It is true that certain GPs (Anti GBM GN, SLE, Post infectious GN, Henoch Schonlein, MPGN, IgA GN, Vasculitis, Cryoglobulinemia, Membranous GN) are more frequently complicated with a high % of crescents than others. What is difficult to understand is that if the presence of CRs is a sign of aggressive disease, why a GP (including the GP listed above) with lower number of CRs should be ignored? especially, when there is no consensus on what is the % of glomeruli involved in a GP to call it CRGN. A descriptive report facilitates de morphologic diagnosis of GP with CRs, standardizes the report of the pathologist, does not interfere with the clinical nomenclature and concepts and does not presume etiology or pathogenesis of the CRs. Finally it gives the clinician freedom for reaching a diagnosis and establishing the prognosis based not only on the pathologists report but also on clinical data and other laboratory tests (ANCA, anti GBM ab, ASO titers, anti nuclear ab, others) and using the clinical nomenclature of his preference. REFERENCES:
2. Colwin HL, Schwartz MM, Lewis EJ: The importance of sample size in the interpretation of renal biopsies. Am J Nephrol 8:85-89, 1996. 3. Falk RJ, Nachman PH, Hogan SL, Jennette JC. ANCA glomerulonephritis and vasculitis: a Chapel Hill perspective. Semin Nephrol 2000 May;20(3):233-43 4. Gal AA, Velasquez A: Antineutrophil Cytoplasmic Autoantibody in the absence of Wegener's granulomatosis or microscopic polyangiatis: Implications for the Surgical Pathologist. Mod Pathol 2002;15(3):197-204. 5. Heptinstall, RH: Pathology of the Kidney. Little, Brown and Company, Boston, 1992. 6. Hoffmann EO: Renal Pathology. https://www.lsuhsc.edu/no/schools/ms/departments/pathology/pathist/dx_home.html 7. Molloy, Peter: ANCA and associated diseases: Update. PSA Consult, Vol. III # 5, May 31, 2000. 8. Moro Rodríguez E, Niembro de Rache E. Síndrome Neumorrenal: Hemorragia pulmonar con glomerulonefritis endo-extracapilar sin evidencia de anticuerpos anti membrana basal glomerular (síndrome Goodpasture probable inmune). Elect. J. Biomed, 1, 2003. Available at: http://biomed.uninet.edu/2003/n1/emoro.html 9. Ordonez NG, Rosai J: Crescentic Glomerulonephritis, Urinary Tract pp 1091. In Rosai J: Ackerman's Surgical Pathology. 8th Ed. Mosby, St Louis 1996. 10. Parmar, MS et al: Glomerulonephritis, Crescentic. eMedicine Pg 2-18. 7/11/2003. Available at: http://www.emedicine.com/MED/topic881.htm 11. Shimazu K, Tomiyoshi Y, Aoki S, Sakemi T, Sugihara H. : Crescentic glomerulonephritis in a patient with heterozygous Fabry's disease. Nephron. 2002 Oct;92(2):456-8. 12. Sorensen SF, Slot O, Tvede N, Petersen J: A prospective study of vasculitis patients collected in a five year period: evaluation of Chapel Hill nomenclature. Ann Rheumatic Dis. 2000 June:59(6):478-82. 13. Striker G, Striker LJ, D'Agaty V: The Renal Biopsy. WB Saunders Co. (3d Ed), Philadelphia 1997. 14. Tisher CC. and Brenner BM: Renal Pathology. JB Lippincott Company, Philadelphia 1994. 15. Wang HJ, Kjellstrad CM, Cockfield SM, Solez K: On the influence of sample size on the prognostic accuracy and reproducibility of renal transplant biopsy. Nephrol Dial Transplant 13:165-172, 1995. November 2003. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||