
|
Paneles de Discussión
Paneais de Discussio Comunicaciones libres
Comunicaçoes livres |
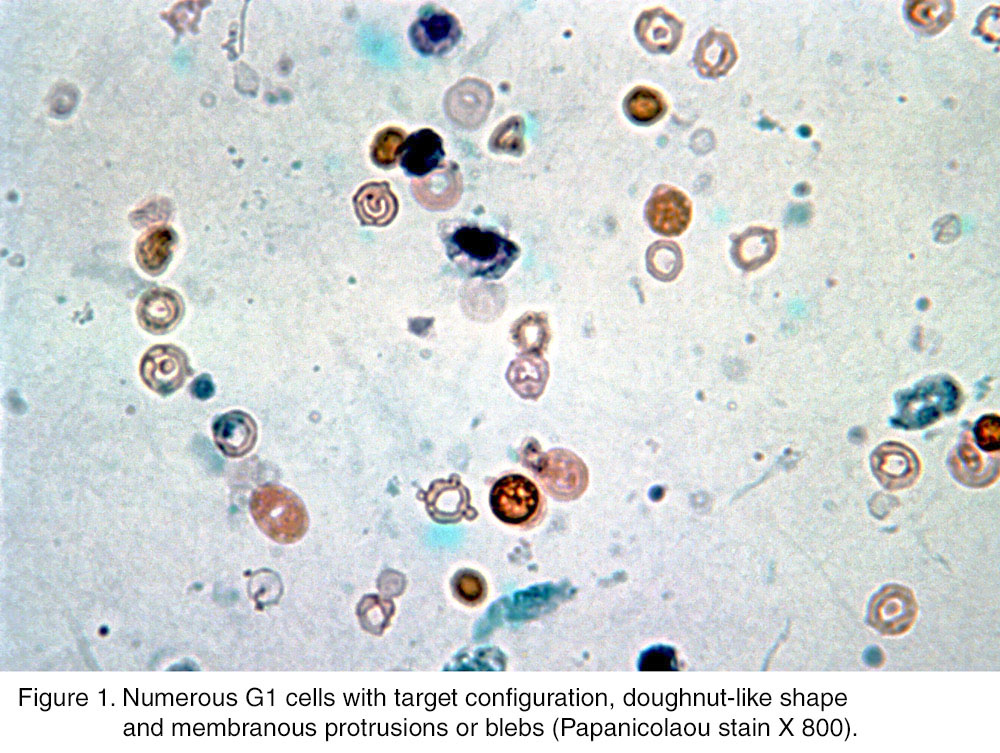
"URINE CYTOLOGY IN RENAL GLOMERULAR DISEASE AND VALUE OF G1 CELL IN THE DIAGNOSIS OF GLOMERULAR BLEEDING"Gia-Khanh Nguyen, M.D., F.I.A.C.Head of Cytopathology, University of Alberta Hospitals, Edmonton, Alberta, Canada.knguyen@cha.ab.caINTRODUCTION Diagnosis of microscopic renal glomerular hematuria is one of the major problems in nephrology, and several studies have been conducted on urine sediments to identify erythrocytes of glomerular origin. Birch and Fairley were the first investigators who have reported that erythrocytes leaking from renal glomeruli were dysmorphic, in contrast to normal erythrocytes of non-glomerular origin 1. This finding proved to be of value in identifying patients with glomerular bleeding in some studies 2-5. However, other studies failed to demonstrate either a high sensitivity or specificity of urinary dysmorphic erythrocytes as an indicator for glomerular bleeding 6,7. In recent years, G1 cells or urinary erythrocytes with doughnut-like shape, target configuration and membranous protrusions or blebs have been reported by Tomita et al. 8 and by other investigators as a reliable marker for glomerular hematuria 9-11. In this lecture, the urine cytology of patients with renal glomerular diseases and the value of G1 cells in the diagnosis of glomerular bleeding will be briefly reviewed
Urine cytology in renal glomerular diseases is best studied by semiquantitative cytologic urinalysis, as the specimen preparation method used in this diagnostic procedure concentrates urinary cellular elements and makes them more easily to be evaluated. For semiquantitative cytologic urinalysis, an aliquot of 10 mL of freshy voided urine without ethanol fixatives is centrifuged at 1800 rpm for 10 min. Nine mL of the supernatant is discarded, and 4 cytospin smears are prepared from the remaining 1 mL of the sediment. The smears obtained are immediately fixed in 95% ethanol for five minutes and then stained by the Papanicolaou method 12. The smears are first screened with a x 10 objective and then selected cellular areas are carefully evaluated in high-power-fields (HPF), using a x 40 objective. Different cellular elements and casts are identified and semiquantitated. G1 cells or G1 dysmorphic erythrocytes are defined as distorted erythrocytes with doughnut-like shape, membranous protrusions or blebs and target configuration with or without membranous blebs 8-11. Other distorted or dysmorphic erythrocytes without the morphologic changes as seen in G1 cells and normal erythrocytes are collectively grouped under the category of non-G1 erythrocytes. The G1 cell/total erythrocyte ratios are calculated by evaluating 200 erythrocytes including G1 cells and non-G1 erythrocytes. In our recent study consisting of 174 patients with histologically confirmed renal glomerular diseases and semiquantitative cytologic urinalyses, the findings in those patients' urine sediments were divided into 4 cytomorphologic groups 13:
1. Abundant G1 cells and non-G1 erythrocytes, and no erythrocytic casts. This type of cytologic manifestation was present in 95 patients (54.6%) who had different types of glomerular disease with IgA and proliferative glomerulonephritis being the most common ones followed by lupus nephritis, thin basement membrane glomerular disease, focal glomerular sclerosis, membranoproliferative glomerulonephritis, minimal change glomerular disease and necrotizing vasculitis, etc 13. About 100 to 200 G1 cells and non-G1 erythrocytes were present in every 10 HPFs (Slide 1). The number of renal tubular cells varied from 20 to 60 per 10 HPFs, consistent with a mild renal tubular injury 12. The amount of lysed erythrocytes or coarsely granular hemoglobin was minimal or absent, and the G1 cell/total erythrocyte ratios in these cases were high and ranged from 80 to 100% 13. Slide 1
3.Abundant erythrocytic casts and non-G1 erythrocytes, and no G1 cells. This cytologic pattern was present in 31 patients (17.8%) with different types of glomerular lesion with proliferative glomerulonephritis being the most common one followed by diabetic nephropathy, focal glomerular sclerosis, membranoproliferative glomerulonephritis and lupus nephritis, etc,13. In the urine sediments about 100 to 400 non-G1 erythrocytes, numerous erythrocytic casts (> 1 erythrocytic casts per HPF), 20 to 100 renal tubular cells were noted per 10 HPFs, consistent with a mild to moderate renal tubular injury 12. Among the non-G1 erythrocytes, erythrocytes with dysmorphic changes were rarely noted 13. 4.Abundant normal erythrocytes only. This cytologic pattern was seen in 13 patients (7.5%) who had different types of glomerular lesion with proliferative glomerulonephritis being the most common lesion followed by focal glomerular sclerosis and diabetic nephropathy, etc 13. In this group of patients the urine sediments showed an unremarkable number of renal tubular cells with up to 20 cells per 10 HPFs. There were abundant normal erythrocytes with 10 to 20 cells per HPF 13.
1. In 130 patients or 74.7% of all cases (patients in groups 1 and 2) in which G1 cells were present, the G1 cell/total erythrocyte ratios varied from 10 to 100%. Thus, a G1 cell/total erythrocyte ratio greater than 10% was a reliable marker for glomerular bleeding 13. 2. The absence of G1 cells in patients with important glomerular bleeding with numerous erythrocytic casts in urine sediments (patients in group 3) could well be attributed to the hemolysis of dysmorphic erythrocytes during their slow passages through the hypotonic renal tubules that were extensively obstructed by numerous erythrocytic casts 13. On the other hand, the presence of numerous G1 cells and non-G1 erythrocytes in urine sediments of patients with less important glomerular bleeding, was probably be due to the quick passages of these cells through the hypotonic renal tubules that were not extensively obstructed by erythrocytic casts (patient in group 2) 13. 3. The number of renal tubular cells was increased in 161 patients (92.5%) 13 and was in keeping with a mild or moderate degree of renal tubular injury or damage that is attributed to the interference of renal tubular vascularization by efferent arterioles in renal glomerular diseases. 4. No specific cytologic manifestations or patterns were found to be associated with any specific types of glomerular disease 13. 5. If the diagnosis of glomerular bleeding was made based only on the presence of abundant erythrocytes and erythrocytic casts without taking into consideration of G1 cell identification, at least 50% of patients with renal glomerular diseases would not be detected by urine cytology.
1. Urinary dysmorphic erythrocytes. Dysmorphic erythrocytes were first described by Becquerel in the 19th century 14. These cells have been of great interest to nephrologists worldwide, and numerous clinical 1-11,15 and experimental studies 15-19 on dysmorphic erythrocytes had been conducted to evaluate their diagnostic value and to explain their pathogenesis. In almost all studies the morphology of urine erythrocytes was evaluated with either a bright-field or a contrast microscope. With these methods of morphologic evaluation the erythrocytes did not show well-defined morphologic details, and as a consequence significant discrepancies existed between observer interpretations of cell morphology; and this explained, in part, the inconsistent results in different studies 1-7. According to some series a diagnosis of glomerular hematuria could be made if numerous dysmorphic erythrocytes were present and the dysmorphic erythrocyte/total erythrocyte ratios were within 60 to 90% ranges 1-5. In our study dysmorphic erythrocytes without morphologic changes as seen in G1 cells were non-specific and had no value in the diagnosis of glomerular bleeding 13. 2. Pathogenesis of urinary dysmorphic erythrocytes. The pathogenesis of dysmorphic erythrocytes is largely unknown. In two studies, the erythrocytes leaked through the diseased renal glomeruli were normal, and these cells acquired dysmorphic changes by osmotic injury while passing through the hypotonic renal tubules and by exposure to acidic and concentrated urine 16, 17. In one study the dysmorphic changes of erythrocytes, in certain cases, were attributed to two consecutive injuries: mechanical injury to the cell membrane during passage through the diseased glomerular basement membrane and osmotic injuries during passage through the hypotonic renal tubules 18. In another study, a combination of a mechanical cell membrane damage, osmotic injury and exposure to acidic urine was necessary to cause dysmorphic changes of erythrocytes 19. 3. Urinary G1 cells. Urinary G1 cells were first described by Tomita et al. in 1992 8. However, erythrocytes with similar morphology had been previously observed in urine samples from patients with glomerulonephritis by Addis in 1948 20 and by Kohler et al. in 1991 15. The latter investigators had named those cells acanthocytes and found that an acanthocyte/total erythrocyte ratio equal or greater than 5% was an evidence for glomerular bleeding/lesion 15. This finding was supported by the work of Kitamoto et al who have demonstrated that a G1 cell/total erythrocytes ratio greater than 5% constituted an evidence for glomerular bleeding 9. In other studies many dysmorphic erythrocytes with morphological changes similar to those of G1 cells had been described and/or illustrated, and these cells and other distorted erythrocytes had been collectively named as dysmorphic erythrocytes 1-5, 21. Despite numerous studies on dysmorphic erythrocytes in the past 25 years the morphological criteria of these cells had not been defined, and the required percentage of these cells for making a firm diagnosis of glomerular bleeding had not been uniform 1-7, 21. G1 cells, on the other hand, are easily identifiable 8-11,13. No G1 cells have been detected in urine sediments of normal individuals and patients with urolithiasis, renal tubular injuries and urothelial neoplasias without associated renal glomerular diseases 22. 4. Pseudo-G1 Cells. Urinary erythrocytes of non-glomerular origin may occasionally showed artefactual changes with target configuration. These cells were named pseudo-G1 cells in our previous study 13. Pseudo-G1 cells showed a well-defined outer hemoglobin rim and a uniformly centrally or eccentrically located hemoglobin mass, and almost all erythrocytes present on the same smear displayed similar morphologic changes (Slide 2). No membranous fragmentation and irregular cell contours, as observed in G1 cells, were noted in pseudo-G1 cells; and an admixture of different types of G1 cells (G1 cells with membranous blebs, doughnut-shape and target configuration) was not observed. The mechanism of pseudo-G1 cell formation was unknown 13. Slide 2

Urinary G1 cells and ECs are important makers for renal glomerular bleeding/disease. Microscopic hematuria is a common clinical finding, and investigation of microhematuria is costly, time-consuming and inconvenient to the patient. A separation of hematuria of glomerular origin from that of a lower urinary tract origin will direct the patient to either a nephrologic or urologic investigation 13. Acknowledgements: Wiley-Liss, Inc, a Wiley Company, has kindly granted the permission for reusing some data and small parts of the article entitled "Urine cytology in renal glomerular disease and value of G1 cell in the diagnosis of glomerular bleeding" that was recently published in Diagnostic Cytopathology 2003, 29:67-73, for this lecture.
REFERENCES
2. Fassett RG, Hogan B, Matthew TH. Detection of glomerular bleeding by phase-contrast microscopy. Lancet 1982; 1:1432-1434
3. Funfstuck R, Schuster FX, Stein G, Beintker M, Schramek P, Jana U. The significance of erythrocyte morphology in glomerular and non-glomerular hematuria. Z Urol Nephrol 1989; 82:85-91
4. Pollock C, Liu PL, Gyory AZ, Grigg R, Gallery ED, Caterson R, Ibels L, Mahoney J, Waugh D. Dysmorphism of urinary red blood cells-value in diagnosis. Kidney Int 1989; 36: 1045-1049
5. Mohammad KS, Bdesha AS, Snell ME, Witherow RO, Coleman DV. Phase contrast microscopic examination of urinary erythrocytes to localise source of bleeding: an overlook technique? J Clin Pathol 1993; 46:642-645
6. Favaro S, Bonfante L, D'Angelo A, Giacomini A, Normanno M, Calo L, Bordin V, Vianello D, Meani A, Antonello A, Borsatti A. Is the red cell morphology really useful to detect the source of hematuria? Am J Nephrol 1997; 17:172-175
7. Ward JF, Kaplan GW, Mevorach R, Stock JA, Cilento BG Jr. Refined microscopic urinalysis for red blood cell morphology in the evaluation of asymptomatic microscopic hematuria in pediatric population. J Urol 1998; 1998; 160:1492-1495
8. Tomita M, Kitamoto Y, Nakayama M, Sato T. A new morphological classification of urinary erythrocytes for differential diagnosis of glomerular hematuria. Clin Nephrol 1992; 37:84-89
9. Kitamoto Y, Tomita M, Akamine M, Inuoe T, Itoh J, Takamori H, Sato T. Differentiation of hematuria using unique shaped red cell. Nephron 1993; 64:32-36
10. Lettgen B, Wohlmuth A. Validity of G1-cells in the differentiation between glomerular and non-glomerular haematuria in children. Pediatr Nephrol 1995; 9:435-437
11. Dinda AK, Saxena S, Guleria S, Tiwari SC, Dash SC, Srivata RN, Singh C. Diagnosis of glomerular haematuria: role of dysmorphic red cell, G1 cell and bright-field microscopy. Scand J Clin Lab Invest 1997; 57:203-208
12 Schumann GB. Cytodiagnostic urinalysis for the nephrology practice. Sem in Nephrol 1986, 6: 308-345
13. Nguyen GK. Urine cytology in renal glomerular disease and value of G1 cell in the diagnosis of glomerular bleeding. Diagn Cytopathol 2003; 29: 67-73
14. Fogazzi GB, Cameron JS, Ritz E, Ponticelli C. The history of urinary microscopy to the end of the 19th century. Am J Nephrol 1994; 14:452-457
15. Kohler H, Wandel E, Brunck B. Acanthocyturia-A characteristic marker for glomerular bleeding. Kidney Int 1991; 40:115-120
16. Schramek P, Moritsch A, Haschkowitz H, Binder BR, Maier M. In vitro generation of dysmorphic erythrocytes. Kidney Int 1989; 36:72-77
17. Kitamoto Y, Yide C, Tomita M, Sato T. The mechanism of glomerular dysmorphic red cell formation in the kidney. Tohoku J Exp Med 1992; 167:93-105
18. Rath B, Turner C, Hartley B, Chantler C. What makes red cells dysmorphic in glomerular hematuria ?. Pediatr Nephrol 1992; 6:424-427
19. Ye RG, Mao XL. Mechanism of urinary erythrocyte deformity in glomerular diseases. Zhonghua Nei Ke Za Zhi 1994; 33:77-79
20. Addis T. Glomerular nephritis. New York: The Mac Millan Co, 1948: 42
21. Fassett RG, Owen JE, Fairley J, Birch DF, Fairley KF. Urinary red cell morphology during exercise. Br Med J (Clin Res Ed) 1986; 285(6353):1455-1457
22. Mireau JR, Smith R, Rayner D, Nguyen GK. Value of G1 cell in the diagnosis of renal glomerular microhematuria. Viet Med J 2002;2:15-20
|