|
Discussion Board
Paneles de Discussi¾n
Paneais de Discussio
Free Papers
Comunicaciones libres
Comunicaþoes livres
Home cin2003
Volver al Inicio cin2003
Voltar ao inicio cin2003
|
Long-Term Survival on Peritoneal Dialysis in End-Stage Renal Disease Due to Diabetes
Ploumis Passadakis1, Vassilis Vargemezis1, Dimitrios Oreopoulos2
(1) Department of Nephrology, Medical School, Democritus University of Thrace, Greece; and
(2) University Health Sciences, The Toronto Western Hospital and University of Toronto,
Toronto, Ontario, Canada
Introduction
Diabetes mellitus is the fastest growing cause of end-stage renal disease (ESRD). Among patients requiring renal replacement therapy (RRT) worldwide, diabetes has become the leading cause of ESRD. Between 1984 and 1997, the percentage of new patients starting RRT whose ESRD was due to diabetes increased from 27% to 42.9% in United States [1].
The first and two-year mortality for diabetic patients in PD between the years 1989 to 1998 have been decreased by 26.6% and 20% per 1000 patient years, respectively [1]. Similar improvement has also been observed in our diabetic patient population in Toronto [2]. However long-term mortality rates in diabetic patients are still twice as high as in nondiabetic dialysis patients and actuarial rates of patient and only a small number of diabetic patients on PD have been followed for more than 5 years.
This may be due to that diabetic patients are vulnerable to considerable morbidity, which has been linked to diabetic nephropathy neuropathy and retinopathy. These devastating complications that increase with age and duration of diabetes as well as the presence of various comorbid conditions at the start of dialysis, may increase diabetic patientsÆ morbidity and mortality rates.
Comorbidity at the initiation of dialysis
Diabetics are at a higher risk of developing concurrent illnesses than the general population, while among ESRD patients, comorbidity is more common in diabetic than in nondiabetic patients. The presence, at the initiation of RRT, of a variety of comorbid conditions such as peripheral vascular disease, cerebrovascular disease, cardiovascular disease, hypoalbuminemia and hyperparathyroidism, may adversely affect outcomes and increase the mortality of diabetic patients undergoing dialysis.
Technique Survival Results of diabetic patients on PD
Although peritonitis remains the major cause of "drop out" (discontinuation of CAPD) among all CAPD patients, there is no evidence that diabetic patients are at increased risk of peritonitis and catheter-related infection. In our study [2], technique survival rates for the first, third, and fifth year of CAPD treatment were 93%, 72%, and 44% respectively; type 1 diabetic patients had better technique survival than type 2 diabetic patients.
Survival of diabetic patients on CAPD
The published [2û15] short-term survival rates for diabetic PD patients range from 74% û 95% (mean: 85%) for the first year, 52% û 84% (mean: 71%) for the second year, and 37% û 72% (mean: 51%) for the third year. After the third year, the reported [2û4,6û12,15] survival rates for diabetic patients on CAPD vary from 17% û 72% (mean: 39%) for the fourth year of survival and from 19% û 63% (mean: 35%) for the fifth year (Figure 1). These values are markedly lower than those of non-diabetic patients undergoing CAPD (Figure 2).
Figure 1. Actuarial patients survival. Long-term survival (beyond four years) of CAPD patients with diabetes mellitus. On the right the references from which the data were obtained are presented. Some of the values were estimated from the graphical presentation from the references.
Figure 2 . Actuarial patients survival. Long-term survival (beyond four years) of non-diabetic CAPD patients. On the right the references from which the data were obtained are presented. Some of the values were estimated from the graphical presentation from the references.
Survival comparison of diabetic ESRD patients on PD and HD
Numerous studies of dialysis populations with varying proportions of diabetic patients attempted to compare long-term clinical outcomes between PD and HD. Despite a disparity in results, most medium and long-term studies concluded that the overall survival rates of patients undergoing peritoneal dialysis and hemodialysis are not statistically significantly different [4,16û19]. Other studies favoured HD [20û22] or PD [23û25], (Table I). It must be noted that whenever an adjustment was made for comorbid factors, the comparison between the two dialysis modalities either showed no statistically significant difference or favoured CAPD.
Table 1. Comparison of long-term survival between continuous ambulatory peritoneal dialysis (CAPD) and hemodialysis (HD), from studies including varying proportions of CAPD diabetic patients
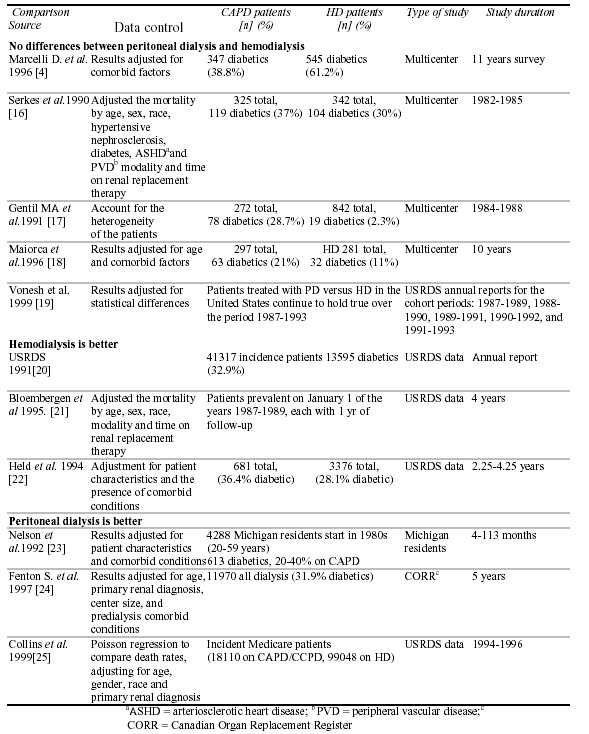
Collins et al [25] evaluated incident Medicare patients from 1994û1996. They used Poisson regression and compared death rates, adjusting for age, sex, race, and primary renal diagnosis. They showed that CAPD/CCPD patients have outcomes comparable to or significantly better than HD patients, although results varied with time. The Cox regression showed a lower mortality in diabetic patients less than 55 years of age on PD (either CAPD or CCPD) than on HD. In contrast, the risk of death (all causes) for female patients with diabetes who were 55 years of age and over was 1.21 for CAPD/CCPD; the risk was lower (1.03) in male patients 55 years of age and over. A more recent reanalysis by Krishnan [26] of the HD versus PD mortality in Canada showed that the previously reported results were holding true over the period from 1990 to 1998 with 7,581 patients on PD and 18,031 on HD. The overall adjusted mortality rate ratio (RR) for PD relative to HD was 0.85 (95% CI 0.81 û 0.89), whereas for the diabetic patients the differences were significant only for younger (< 64 years) males (RR 0.80 (0.71 û 0.91)). Diabetic females on PD had a significantly higher mortality rate than males in both age groups, whereas in non-diabetic females on PD the significantly higher mortality rate than males was seen in the │ 65 years age group.
In general comparisons of clinical outcomes in HD and PD diabetic patients have been marked by inconsistent results depending on the population studied and the methods used.
Conclusion
Although several clinical studies have evaluated the factors affecting survival rates of diabetic dialysis patients, only a few studies have followed diabetic PD patients for more than five years. Moreover, despite the more sophisticated statistical methods being used to compare survival rates -either for diabetic patients between the two major dialysis modalities, or between CAPD patients with and without diabetes-methods and patient selection biases conceal potential problems, influence results, and make comparisons difficult. The higher incidence of multiple comorbid factors at dialysis initiation, older age, nutritional status, and technique limitations over the long-term (such as episodes of peritonitis, ultrafiltration "failure," loss of residual renal function, inadequate dialysis, and the peritoneal membrane failure) may shorten PD longevity in ESRD patients with diabetes mellitus undergoing CAPD. However, as long as the peritoneal membrane maintains its ability to adequately purify blood for a long time, CAPD remains a viable form of long-term renal replacement therapy for diabetic patients with end-stage renal disease.
References
1.U.S. Renal Data System, USRDS 2001 Annual Data Report: Atlas of End-Stage Renal Disease in the United States, National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, Bethesda, MD, 2001.
2.Passadakis P, Oreopoulos DG. Continuous ambulatory peritoneal dialysis in 224 diabetics with end stage renal disease: Evidence of improved survival over the past 10 years. In: Friedman EA, LÆEsperance FA, eds. Diabetic renal-retinal syndromeù21st century management now. Boston: Kluwer Academic Publishers; 1998: 89û115.
3.Viglino G, Cancarini GC, Catizone L, et al. Ten years experience of CAPD in diabetics: Comparison of results with non-diabetics. Nephrol Dial Transplant 1994; 9:1443û8.
4.Marcelli D, Spotti D, Conte F, et al. Survival of diabetic patients on peritoneal dialysis or hemodialysis. Perit Dial Int 1996; 16(Suppl 1):S283û7.
5.Zimmerman SW, Oxton LL, Bidwell D, Wakeen M. Long-term outcome of diabetic patients receiving peritoneal dialysis. Perit Dial Int 1996; 16:63û8.
6.Coronel F, Hortal L, Naranjo P, et al. Analysis of factors in the prognosis of diabetics on continuous ambulatory peritoneal dialysis (CAPD): Long-term experience. Perit Dial Int 1989; 9:121û5.
7.Kemperman FA, van Leusen R, van Liebergen FJ, et al. Continuous ambulatory peritoneal dialysis (CAPD) in patients with diabetic nephropathy. Neth J Med 1991; 38:236û45.
8.McMillan MA, Briggs JD, Junor BJ. Outcome of renal replacement treatment in patients with diabetes mellitus. BMJ 1990; 301(6751):540û4.
9.Catalano C, Goodship TH, Tapson JS, et al. Renal replacement treatment for diabetic patients in Newcastle upon Tyne and the northern region, 1964û88. BMJ 1990; 301(6751):535û40.
10.Rotellar C, Black J, Winchester JF, et al. Ten yearsÆ experience with continuous ambulatory peritoneal dialysis. Am J Kidney Dis 1991; 17(2):158û64.
11.Lupo A, Tarchini R, Cancarini G, et al. Long-term outcome in continuous ambulatory peritoneal dialysis: A 10-year survey by the Italian Cooperative Peritoneal Dialysis Study Group. Am J Kidney Dis 1994; 25(5):826û37.
12.Rodriguez JA, Cleries M, Vela E. Diabetic patients on renal replacement therapy: Analysis of Catalan Registry data. Nephrol Dial Transplant 1997; 12(12):2501û9.
13.Zimmerman SW, Glass N, Sollinger H, Miller D, Belzer F. Treatment of end-stage diabetic nephropathy: Over a decade of experience at one institution. Medicine (Baltimore) 1984; 63(5):311û17.
14.Rottembourg J, Issad B, Allouache M, et al. Clinical aspects of continuous ambulatory peritoneal dialysis in diabetics. Nephrologie 1988; 9(5):227û32.
15.Miles AM, Friedman EA. Dialytic therapy for diabetic patients with terminal renal failure. Curr Opin Nephrol Hypertens 1993; 2(6):868û75.
16.Serkes KD, Blagg CR, Nolph KD, Vonesh EF, Shapiro F. Comparison of patient and technique survival in continuous ambulatory peritoneal dialysis (CAPD) and hemodialysis: A multicenter study. Perit Dial Int 1990; 10:15û19.
17.Gentil MA, Carriazo A, Pavon MI, et al. Comparison of survival in continuous ambulatory peritoneal dialysis and hospital haemodialysis: A multicentric study. Nephrol Dial Transplant 1991; 6:444û51.
18. Maiorca R, Cancarini GC, Zubani R, et al. CAPD viability: A long-term comparison with hemodialysis. Perit Dial Int 1996; 16(3):276û87.
19.Vonesh EF, Moran J. Mortality in end-stage renal disease: A reassessment of differences between patients treated with hemodialysis and peritoneal dialysis. J Am Soc Nephrol 1999; 10:354û65.
20.United States Department of Health and Human Services, Public Health Service, National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases. USRDS 1991 Annual Data Report. Am J Kidney Dis 1991; 18(Suppl 2): 49û60.
21.Bloembergen WE, Port FK, Mauger EA, Wolfe RA. A comparison of mortality between patients treated with hemodialysis and peritoneal dialysis. J Am Soc Nephrol 1995; 6(2):177û83.
22.Held PJ, Port FK, Turenne N, Gaylin DS, Hamburger RJ, Wolfe RA. Continuous ambulatory peritoneal dialysis and hemodialysis: Comparison of patient mortality with adjustment for comorbid conditions. Kidney Int 1994; 45:1163û9.
23.Nelson CB, Port FK, Wolfe RA, Guire KE. Comparison of continuous ambulatory peritoneal dialysis and hemodialysis patient survival with evaluation of trends during the 1980s. J Am Soc Nephrol 1992; 3:1147û55.
24.Fenton SS, Schaubel DE, Desmeules M, et al. Hemodialysis versus peritoneal dialysis: A comparison of adjusted mortality rates. Am J Kidney Dis 1997; 30:334û42.
25.Collins AJ, Hao W, Xia H, et al. Mortality risks of peritoneal dialysis and hemodialysis. Am J Kidney Dis 1999; 34(6):1065û74.
26.Krishnan M, Schaubel D, Bargman M J, Oreopoulos D G, Fenton SSA.HD versus PD in Canada Revised. Abstract, Meeting of the International Society of Nephrology, Montreal, June 26-28, 2001.
Corresponding author:
Ploumis S. Passadakis, MD,
26 Vizvizi Street, Alexandroupolis, Greece.
ploumis@hol.gr
|
