1.Libby P, Ridker PM, Maseri A. Inflammation and atherosclerosis. Circulation 2002; 105: 1135-42
2.Foley RN, Parfrey PS, Sarnak MJ. Clinical epidemiology of cardiovascular disease in chronic renal disease. Am-J-Kidney-Dis 1998; 32: S112-9
3.Bologa RM, Levine DM, Parker TS, et al. Interleukin-6 predicts hypoalbuminemia, hypocholesterolemia, and mortality in hemodialysis patients. American Journal Of Kidney Diseases 1998; 32 (1): 107-14
4.Zimmermann J, Herrlinger S, Pruy A, Metzger T, Wanner C. Inflammation enhances cardiovascular risk and mortality in hemodialysis. Kidney Int 1999; 55: 648-58
5.Haubitz M, Brunkhorst R, Wrenger E, Froese P, Schulze M, Koch KM. Chronic induction of C-reactive protein by hemodialysis, but not by peritoneal dialysis therapy. Perit-Dial-Int 1996; 16: 158-62
6.Stenvinkel P. Inflammation in end-stage renal disease: could it be treated? Nephrol Dial Transplant 2002; 17: 33-8
7.Oppermann M, Kurts C, Zierz R, Quentin E, Weber M, Gotze O. Elevated plasma levels of the immunosuppressive complement fragment Ba in renal failure. Kidney Int 1991; 40: 939-47
8.Poole S, Bird TA, Selkirk S, et al. Fate of injected interleukin 1 in rats: sequestration and degradation in the kidney. Cytokine 1990; 2: 416-22
9.Andersen SR, Lambrecht LJ, Swan SK, et al. Disposition of recombinant human interleukin-10 in subjects with various degrees of renal function. J CLIN PHARMACOL. Journal of Clinical Pharmacology 1999; 39: 1015-20
10.Descamps Latscha B, Herbelin A, Nguyen AT, et al. Balance between IL-1 beta, TNF-alpha, and their specific inhibitors in chronic renal failure and maintenance dialysis. Relationships with activation markers of T cells, B cells, and monocytes. J Immunol 1995; 154: 882-92
11.Schindler R, Boenisch O, Fischer C, Frei U. Effect of the hemodialysis membrane on the inflammatory reaction in vivo. Clin-Nephrol 2000; 53: 452-9
12.Miyata T, Hori O, Zhang J, et al. The receptor for advanced glycation end products (RAGE) is a central mediator of the interaction of AGE-beta2microglobulin with human mononuclear phagocytes via an oxidant-sensitive pathway. Implications for the pathogenesis of dialysis-related amyloidosis. J Clin Invest 1996; 98: 1088-94
13.Witko-Sarsat V, Friedlander M, Khoa TN, et al. Advanced oxidation protein products as novel mediators of inflammation and monocyte activation in chronic renal failure. J Immunol 1998; 161: 2524-32
14.Bergstrom J, Wang T, Lindholm B. Factors contributing to catabolism in end-stage renal disease patients. Miner Electrolyte Metab 1998; 24: 92-101
15.Williams B, Layward E, Walls J. Skeletal muscle degradation and nitrogen wasting in rats with chronic metabolic acidosis. Clin Sci 1991; 80: 457-62
16.Stein A, Moorhouse J, Iles-Smith H, al. e. Role of an improvement in acid-base status and nutrition in CAPD patients. Kidney Int 1997; 52: 1089-95
17.Pickering WP, Price SR, Bircher G, Marinovic AC, Mitch WE, Walls J. Nutrition in CAPD: serum bicarbonate and the ubiquitin-proteasome system in muscle. Kidney-Int 2002; 61: 1286-92
18.Flores EA, Bistrian BR, Pomposelli JJ, Dinarello CA, Blackburn GL, Istfan NW. Infusion of tumor necrosis factor/cachectin promotes muscle catabolism in the rat. A synergistic effect with interleukin 1. J-Clin-Invest 1989; 83: 1614-22
19.Boenisch O, Willam C, Koehne P, Wilde A, Frei U, Schindler R. Acidosis induces and augments gene expression and synthesis of Interleukin-6 and RANTES in smooth muscle cells (abstract). JASN 2001; 12: 133A
20.Niebauer J, Volk HD, Kemp M, et al. Endotoxin and immune activation in chronic heart failure: a prospective cohort study. Lancet 1999; 353: 1838-42
21.Dumler F. Hypoalbuminemia is a marker of overhydration in chronic maintenance patients on dialysis. Asaio J 2003; 49: 282-6
22.Torre Amione G, Kapadia S, Benedict C, Oral H, Young JB, Mann DL. Proinflammatory cytokine levels in patients with depressed left ventricular ejection fraction: a report from the Studies of Left Ventricular Dysfunction (SOLVD). J-Am-Coll-Cardiol 1996; 27: 1201-6
23.Torre Amione G, Kapadia S, Lee J, et al. Tumor necrosis factor-alpha and tumor necrosis factor receptors in the failing human heart. Circulation 1996; 93: 704-11
24.Murray DR, Prabhu SD, Chandrasekar B. Chronic beta-adrenergic stimulation induces myocardial proinflammatory cytokine expression. Circulation 2000; 101: 2338-41
25.Ohtsuka T, Hamada M, Hiasa G, et al. Effect of beta-blockers on circulating levels of inflammatory and anti-inflammatory cytokines in patients with dilated cardiomyopathy. J Am Coll Cardiol 2001; 37: 412-7
26.Himmelfarb J, Lazarus JM, Hakim R. Reactive oxygen species production by monocytes and polymorphonuclear leukocytes during dialysis. Am J Kidney Dis 1991; 17: 271-6
27.Klein JB, McLeish KR, Ward RA. Transplantation, not dialysis, corrects azotemia-dependent priming of the neutrophil oxidative burst. Am-J-Kidney-Dis 1999; 33: 483-91
28.Ward RA, Ouseph R, McLeish KR. Effects of high-flux hemodialysis on oxidant stress. Kidney Int 2003; 63: 353-9
29.Himmelfarb J, Stenvinkel P, Ikizler TA, Hakim RM. The elephant in uremia: oxidant stress as a unifying concept of cardiovascular disease in uremia. Kidney Int 2002; 62: 1524-38
30.Ward RA, McLeish KR. Oxidant stress in hemodialysis patients: what are the determining factors? Artif Organs 2003; 27: 230-6
31.Drueke T, Witko Sarsat V, Massy Z, et al. Iron therapy, advanced oxidation protein products, and carotid artery intima-media thickness in end-stage renal disease. Circulation 2002; 106: 2212-7
32.Craddock PR, Fehr J, Dalmassso AP, Brigham KL, Jacob HS. Hemodialysis leukopenia: pulmonary vascular leukostasis resulting from complement activation by dialyzer cellophane membranes. J Clin Invest 1977; 59: 879-88
33.Schindler R, Linnenweber S, Schulze M, et al. Gene expression of interleukin-1 beta during hemodialysis. Kidney Int 1993; 43: 712-21
34.Hoerl WH. Hemodialysis membranes: interleukins, biocompatibility and middle molecules. JASN 2002; 13: S62-S71
35.Tayeb JS, Provenzano R, El Ghoroury M, et al. Effect of biocompatibility of hemodialysis membranes on serum albumin levels. Am-J-Kidney-Dis 2000; 35: 606-10
36.Memoli B, Minutolo R, Bisesti V, et al. Changes of serum albumin and C-reactive protein are related to changes of interleukin-6 release by peripheral blood mononuclear cells in hemodialysis patients treated with different membranes. Am-J-Kidney-Dis 2002; 39: 266-73
37.Laude-Sharp M, Haeffner CN, Caroff M, Lantreibecq F, Pusineri C, Kazatchkine MD. Dissociation between the interleukin 1-inducing capacity and Limulus reactivity of lipopolysaccharides from gram-negative bacteria. Cytokine 1990; 2: 253-8
38.Krautzig S, Linnenweber S, Schindler R, Shaldon S, Koch KM, Lonnemann G. New indicators to evaluate bacteriological quality of the dialysis fluid and the associated inflammatory response in ESRD patients. Nephrol Dial Transplant 1996; 2: 87-91
39.Lonnemann G, Schindler R, Lufft V, Mahiout A, Shaldon S, Koch KM. The role of plasma coating on the permeation of cytokine-inducing substances through dialyser membranes. Nephrol Dial Transplant 1995; 10: 207-11
40.Stacey KJ, Sweet MJ, Hume DA. Macrophages ingest and are activated by bacterial DNA. J-Immunol 1996; 157: 2116-22
41.Krieg AM. CpG motifs in bacterial DNA and their immune effects. Annu Rev Immunol 2002; 20: 709-60
42.Ballas ZK, Rasmussen WL, Krieg AM. Induction of NK activity in murine and human cells by CpG motifs in oligodeoxynucleotides and bacterial DNA. J-Immunol 1996; 157: 1840-5
43.Verthelyi D, Ishii K, Gursel M, Takeshita F, Klinman D. Human peripheral blood cells differentially recognize and respond to two distinct CPG motifs. J-Immunol 2001; 166: 2372-7
44.Hemmi H, Takeuchi O, Kawai T, et al. A Toll-like receptor recognizes bacterial DNA. Nature 2000; 408: 740-5
45.Pereira BJ, Snodgrass BR, Hogan PJ, King AJ. Diffusive and convective transfer of cytokine-inducing bacterial products across hemodialysis membranes. Kidney-Int 1995; 47: 603-10
46.Lonnemann G, Behme TC, Lenzner B, et al. Permeability of dialyzer membranes to TNF alpha-inducing substances derived from water bacteria. Kidney Int 1992; 42: 61-8
47.Schindler R, Krautzig S, Lufft V, et al. Induction of interleukin-1 and interleukin-1 receptor antagonist during contaminated in-vitro dialysis with whole blood. Nephrol-Dial-Transplant 1996; 11: 101-8
48.Schindler R, Dinarello CA. Ultrafiltration to remove endotoxins and other cytokine-inducing materials from tissue culture media and parenteral fluids. Biotechniques 1990; 8: 408-13
49.Schindler R, Christ-Kohlrausch F, Frei U, Shaldon S. Differences in the permeability of high-flux dialyzer membranes for bacterial pyrogens. Clin Nephrol 2003; 59: 447-54
50.Ayus JC, Sheikh Hamad D. Silent infection in clotted hemodialysis access grafts. J-Am-Soc-Nephrol 1998; 9: 1314-7
51.Jaar BG, Hermann JA, Furth SL, Briggs W, Powe NR. Septicemia in diabetic hemodialysis patients: comparison of incidence, risk factors, and mortality with nondiabetic hemodialysis patients. Am-J-Kidney-Dis 2000; 35: 282-92
52.Pastan S, Soucie JM, McClellan WM. Vascular access and increased risk of death among hemodialysis patients. Kidney-Int 2002; 62: 620-6
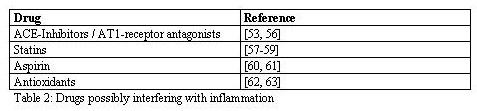
53.Schindler R, Dinarello CA, Koch KM. Angiotensin-converting-enzyme inhibitors suppress synthesis of tumour necrosis factor and interleukin 1 by human peripheral blood mononuclear cells. Cytokine 1995; 7: 526-33
54.Gullestad L, Aukrust P, Ueland T, et al. Effect of high- versus low-dose angiotensin converting enzyme inhibition on cytokine levels in chronic heart failure. J-Am-Coll-Cardiol 1999; 34: 2061-7
55.Stenvinkel P, Andersson P, Wang T, et al. Do ACE-inhibitors suppress tumour necrosis factor-alpha production in advanced chronic renal failure? J-Intern-Med 1999; 246: 503-7
56.Tsutamoto T, Wada A, Maeda K, et al. Angiotensin II type 1 receptor antagonist decreases plasma levels of tumor necrosis factor alpha, interleukin-6 and soluble adhesion molecules in patients with chronic heart failure. J-Am-Coll-Cardiol 2000; 35: 714-21
57.Kinlay S, Timms T, Clark M, et al. Comparison of effect of intensive lipid lowering with atorvastatin to less intensive lowering with lovastatin on C-reactive protein in patients with stable angina pectoris and inducible myocardial ischemia. Am-J-Cardiol 2002; 89: 1205-7
58.Ridker PM, Rifai N, Lowenthal SP. Rapid reduction in C-reactive protein with cerivastatin among 785 patients with primary hypercholesterolemia. Circulation 2001; 103: 1191-3
59.Chang JW, Yang WS, Min WK, Lee SK, Park JS, Kim SB. Effects of simvastatin on high-sensitivity C-reactive protein and serum albumin in hemodialysis patients. Am-J-Kidney-Dis 2002; 39: 1213-7
60.Ikonomidis I, Andreotti F, Economou E, Stefanadis C, Toutouzas P, Nihoyannopoulos P. Increased proinflammatory cytokines in patients with chronic stable angina and their reduction by aspirin. Circulation 1999; 100: 793-8
61.Feldman M, Jialal I, Devaraj S, Cryer B. Effects of low-dose aspirin on serum C-reactive protein and thromboxane B2 concentrations: a placebo-controlled study using a highly sensitive C-reactive protein assay. J-Am-Coll-Cardiol 2001; 37: 2036-41
62.Devaraj S, Jialal I. Alpha tocopherol supplementation decreases serum C-reactive protein and monocyte interleukin-6 levels in normal volunteers and type 2 diabetic patients. Free-Radic-Biol-Med 2000; 29: 790-2
63.Bruunsgaard H, Poulsen HE, Pedersen BK, Nyyssonen K, Kaikkonen J, Salonen JT. Long-term combined supplementations with alpha-tocopherol and vitamin C have no detectable anti-inflammatory effect in healthy men. J Nutr 2003; 133: 1170-3
64.Murray DR, Freeman GL. Proinflammatory cytokines: predictors of a failing heart? Circulation 2003; 107: 1460-2
65.Sato Y, Takatsu Y, Kataoka K, et al. Serial cirulating concentrations of c-reactive protein, interleukin-4 and IL-6 in patients with acute left heart decompensation. Clin Cardiol 1999; 22: 811-3
66.Kooistra MP, Kersting S, Gosriwatana I, et al. Nontransferrin-bound iron in the plasma of haemodialysis patients after intravenous iron saccharate infusion. Eur J Clin Invest 2002; 1: 36-41
67.Klein E, Pass T, Harding GB, Wright R, Million C. Microbial and endotoxin contamination in water and dialysate in the central united states. Artif Organs 1990; 14: 85-94
68.Lonnemann G. The quality of dialysate: an integrated approach. Kidney Int Suppl 2000; 76: S112-9
69.Nassar GM, Ayus JC. Infectious complications of old nonfunctioning arteriovenous grafts in renal transplant recipients: a case series. Am-J-Kidney-Dis 2002; 40: 832-6

 and soluble TNF-receptors rise with the severity of renal failure and correlate with GFR [10].
and soluble TNF-receptors rise with the severity of renal failure and correlate with GFR [10]. 
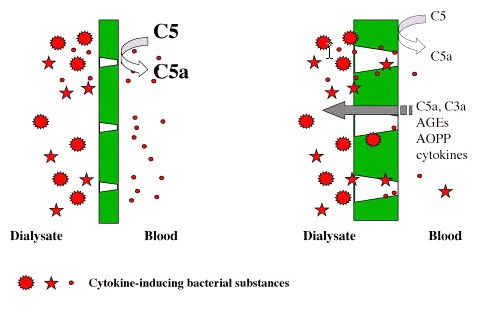
 and IL-6 while HD with non-complement-activating membranes express much less mRNA for these cytokines [33].
and IL-6 while HD with non-complement-activating membranes express much less mRNA for these cytokines [33].
 , TNF-
, TNF- and IL-6 from PBMC [42, 43]. When injected intraperitoneally, CpG ODN induce IL-6, TNF and IL-12 in mice and may even lead to septic shock [44]. The signaling pathways by which CpG ODN activate cells are currently being characterized and involve Toll-like receptor 9 (TLR9).
and IL-6 from PBMC [42, 43]. When injected intraperitoneally, CpG ODN induce IL-6, TNF and IL-12 in mice and may even lead to septic shock [44]. The signaling pathways by which CpG ODN activate cells are currently being characterized and involve Toll-like receptor 9 (TLR9).