Medial thickenings of coronary artery in relation to renal microvasculopathies of hypertension.
Richard E Tracy MD PhD.
Department of Pathology. Louisiana State University. Health Sciences Center.
New Orleans LA. USA
ABSTRACT
Mean blood pressure (MBP) can be estimated by measuring renovasculopathies at autopsy. In this study, MBP was found to correlate with coronary arterial medial thickness. The correlation was found alike in men and women of ages 15-44 years, but not in older ages. A thickened media seemed to convey enhanced risk of atheroma, and the risk was associated entirely with the fibroplastic thickness per SMC and not with SMC numbers. Elevated MBP also seemed to convey enhanced risk of atheroma, and again the risk was associated only with FM and not with SMC numbers. These patterns reproduce previously reported findings on coronary intimal fibroplasia. The outcome suggests that rapid progression of fibroplasia per SMC with age acts to accelerate the onset of atheroma, and that this fibroplasia is a general property of the artery as a whole, affecting media as well as intima. Results are consistent with the view that elevated mean blood pressure may promote coronary atheroma by way of accelerating the underlying fibroplasia of aging. These findings derive from 553 forensic autopsies with kidneys and coronary arteries examined histologically in paraffin sections.
INTRODUCTION
Coronary arteries examined at autopsy reveal a wide range of variation from one specimen to another in average thickness of the medial layer. The arteries with the thickest media were recently shown to experience accelerated progression toward atheroma [1]. Thickening is the product of SMC numbers times the thickness of fibroplastic matrix per SMC; it was the latter, the fibroplasia per SMC, that held an ominous implication for emergence of atheroma while SMC numbers had no such implication. A consideration raised by these findings is that hypertension might act to introduce excessive fibroplasia per SMC, and in this way accelerate progression toward atheroma.
Aging renal interlobular arteries tend to experience a progressive thickening of the intima with dense collagenous layers that accompany wastage and disappearance of the media [2]. This intimal fibroplasia of renal microvessels has a strong correlation with blood pressure. When data are available in a series of autopsies on both variables, blood pressure and renovascular fibroplasia, the hypertensive subjects can be divided into Type 1 and Type 2 [3]. Some hypertensives have mild or minimal renovasculopathy and these are called Type 1. Most elderly hypertensives, however, reveal severe renovasculopathy, and these are called Type 2. When a series of forensic autopsies provide measurements of renovasculopathy (intimal thickness in units of % outer diameter) these data can be entered into a set of equations to calculate expected Type 2 blood pressure levels [2].
By measuring coronary medial thickness and fibroplasia per SMC in a series of autopsies with known Type 2 blood pressure levels (determined from renovasculopathy) it becomes possible to correlate these variables with each other. This approach allows inquiry into the association of hypertension with coronary medial structure.
MATERIALS AND METHODS:
Methods summarized here are described more fully elsewhere [1-3]. Formalin fixed specimens of coronary artery and renal cortex are prepared at autopsy from men and women of black and white ethnic groups aged 15-79 years in the Orleans Parish Coroner’s Office from 1996-2001. Emphasis was given to retaining basal subjects in this series. The basal category comprises subjects dying of violence, or natural causes having no known correlation with hypertension or atherosclerosis, and the basal group offers an approximation to a representative sample of the population. However, this property of the autopsy series is not required for present purposes, and some instances coronary heart disease and other cardiovascular conditions are retained.
The proximal right coronary artery is opened longitudinally, cut into three segments of three cm length each, embedded in paraffin on edge to allow sectioning perpendicular to the luminal surface, and stained with hematoxylin and eosin (H&E). Atheromas are marked in black ink on the cover slip of the coronary artery sections. Arteries having at least one instance of atheroma in the specimen are called YesA, otherwise they are NoA. At nine equally spaced positions along the coronary sample, excluding black marked locations, measurements are taken of medial thickness, counts are made of SMC’s in a 100 :m wide band through the full medial thickness, and the ratio of thickness to SMC’s is calculated. Means of these three variables are called M, CM, and FM respectively. Renal cortex is sectioned in paraffin and stained with PAS-alcian blue.
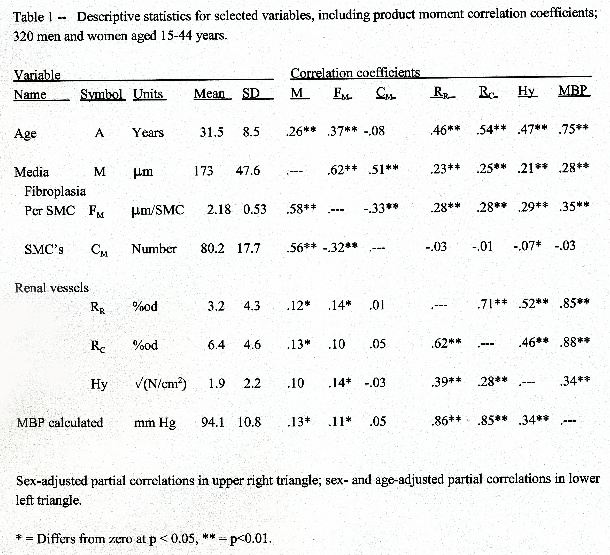
Intimal thickness of renal interlobular arteries is determined as percentage of outer diameter, %od. The averages of these percentages in the size ranges of 80-149 :m and 150-300 :m are called Rr and Rc respectively, standing for renal resistance level and renal conduit level vessels. Numbers of hyalinized arterioles were counted as N per cm2 of observed renal cortex, taking the square root to diminish the skew in the distribution of this variable. Table 1 gives descriptive statistics for the variables of interest; these provide information for multivariate analyses including correlation and regression. Treating mean blood pressure (MBP) as a function of arterial fibroplasia (Rc) and age (A), multiple linear regression allows the determination of an equation that defines the complete cubic response surface:
MBPc = 53.1 + 2.001A - 0.03100A2 + 0.0001352A3 + 1.398Rc + 0.2209Rc2
- 0.003841Rc3 - 0.07451ARc + 0.0007319A2Rc - 0.0008690ARc2
{R2 = 0.493} (1)
A similar equation can be determined using the alternative measure of fibroplasia, Rr,
MBPr = 52.7 + 2.198A - 0.03794A2 + 0.0002059A3 + 2.666Rr + 0.1640Rr2
- 0.003140Rr3 - 0.06789ARr + 0.0006711A2Rr - 0.001197ARr2
{R2 = 0.510} (2)
The final estimate of Type 2 mean pressure is MBP = (MBPc + MBPr)/2. This also is entered in Table 1. Multiple regression is done with the program PROC STEPWISE and discriminant function analysis is done with PROC STEPDISC and PROC DISRIM all provided by SAS inc, Cary NC.
RESULTS:
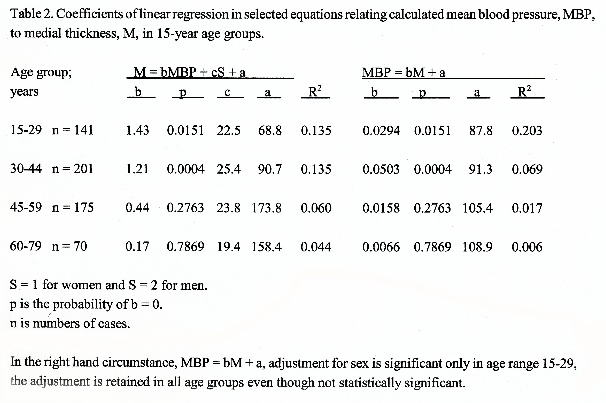
Men revealed average coronary medial thickness about 22 :m greater than women in all age groups from 15-29 to 60-79 years (Table 2). The effect of MBP on medial thickness was alike in the two sexes, without interactions in the regression equations. The increase of medial thickness was about 13 :m per 10 mm Hg MBP at ages 15-44 years, but was not significant after age 44 years. In the younger ages this is about 23 % increased thickness at MBP of 124.1 mm Hg compared with the overall mean of 94.1 mm Hg.
In the pool of subjects aged 15-44 years, the variable CM, numbers of SMC’s per medial site, did not correlate with sex or MBP. The variables M, medial thickness, and FM, fibroplasia per SMC, both correlated with MBP in accordance with the following equations, where age is rejected from Equation 3 as not statistically significant.
M = 0.803MBP + 30.2S + 139 (R2 = 0.125) (3)
FM = 0.00777MBP + 0.130S + 0.0156A (R2 = 0.166) (4)
The standardized coefficients apply when variables are measured in units of their standard deviations; these are M = 0.18MBP + 0.30S and FM = 0.16MBP + 0.11S + 0.25A. These offer assessment of relative importance for each variable, and indicate that MBP is about equally strong when predicting M or FM, whereas CM is of no significance.
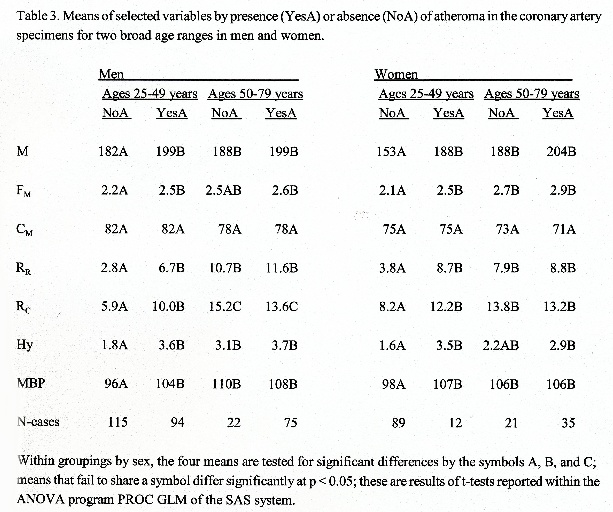
Table 3 reports comparisons of YesA with NoA arteries. At ages 25-49 years, YesA arteries exceeded NoA specimens in M, FM, Rr, Rc, Hy, and MBP but not in CM, and the pattern was the same in men and women. At ages 50-79 years, YesA arteries did not differ from NoA specimens in any of these comparisons.
In a multivariate setting discriminant functions were computed for distinguishing YesA from NoA arteries. Reporting standardized coefficients, each specimen is predicted to be YesA if W > 0 and NoA if W < 0:
W = 0.72MBP + 0.60M + 0.84S + 0.94A - 0.28CM (T2 = 2.08 c = -9.79 OR = 11.8) (5)
T2 is the difference between mean W in the YesA minus NoA cases measured in units of squared standard deviation of W, c is the constant to add when regenerating the raw coefficients using standard deviations from Table 1 (SD for sex is 0.47), and OR is the odds ratio for odds of correct prediction divided by odds of false prediction. The variable CM is not statistically significant, and the equation omitting this is
W = 0.67MBP + 0.45M + 0.86S + 1.03A (T2 = 2.07 c = -10.37 OR = 11.3) (6)
The inclusion of MBP does not displace M and the variable CM does not gain significance in the multivariate setting.
In the pool of ages 50-79 years, Equations 5 and 6 had no significant terms to distinguish YesA from NoA specimens. This lack of significance may be the result of few NoA cases in the series because only 43 cases were encountered.
DISCUSSION:
The level of blood pressure reflected in the variable MBP represents exclusively Type 2 hypertension, because the Type 1 is by definition lacking any correlation with renovasculopathies. However, in pools of subjects, the mean MBP has repeatedly been shown to correlate with observed blood pressures between age groups, populations, and age-specific pools of individuals within populations [3]. Hence, the subjects with high MBP can reliably be viewed as manifesting elevated blood pressure, at least in the group averages. The finding of correlations between MBP and medial thickness could, in theory, arise because of direct action of unknown agents upon arterial structure, both coronary and renal microvasculature, rather than because of an action by blood pressure. Nevertheless, it can be deduced that blood pressure generally tends to be higher in subjects with coronary medial thickening as a provisional conclusion from the data reported here.
Medial thickness, M, is the product of the two variables FM and CM, fibroplasia per SMC and number of SMC’s per site. In all situations, the correlations of MBP with M are paralleled by equivalent correlations with FM whereas no significant correlation emerged between MBP and CM in any circumstance. Hence, the blood pressure linked effect in coronary architecture is unrelated to SMC numbers which remain essentially alike at all levels of blood pressure.
Subjects with atheroma in the coronary specimen, YesA cases, had average MBP much greater than those without atheroma, NoA cases (Table 3). The YesA cases also had greater medial thickness which related to FM but not to CM. These patterns of relationship raise the possibility that elevated blood pressure could accelerate the progression of atheroma by propelling the progression of fibroplasia per SMC. A similar suggestion arose when the intimal layer was examined in a series of coronary arteries [4].
CONCLUSIONS:
Medial architecture of the coronary artery shows a consistent pattern of interrelationships with blood pressure levels assessed indirectly by measurements of renovasculopathies.
The pattern reproduces previous findings for coronary intimal architecture. The outcome suggests that rapid progression of fibroplasia per SMC with age acts to accelerate the onset of atheroma, and that this fibroplasia is a general property of the artery as a whole, affecting media as well as intima.
Results are consistent with the view that elevated mean blood pressure may promote coronary atheroma by way of accelerating the underlying fibroplasia of aging.
REFERENCES:
1. Tracy RE. (2003) Fibroplasia per SMC in the media of coronary arteries. in R.E.Tracy (Ed.) The Role of Aging in Atherosclerosis (Chapter16, pp 165-181). Dordrecht/Boston/London: Kluwer Academic Press.
2. Tracy RE. (1999) Salt, obesity, and alcohol fail to induce a lasting rise of blood pressure with age, and may be independent of renocortical vasculopathy. QJMed 92:601-607.
3. Tracy, R.E., Lanjewar, D.N., Ghorpade, K.G., Valand, A.G., and Raghuwanshi, S.R. (1997) Renovasculopathies of hypertension in Bombay, India. Geriat Nephrol Urol 7:101-4
4. Tracy, R.E. (1998) Histological characteristics of coronary artery in relation to the renovasculopathies of hypertension. Ann Diag Pathol 2:1-9.
|