Basis: ARF is a medical emergency where the outcome depends on early diagnosis and intervention. Diagnosis based on clinical, laboratory and ultrasound examination is still imperfect and renal biopsy remains the only gold standard. Renal biopsy cannot be performed in all situations. Any new noninvasive investigation, increasing the sensitivity and specificity of clinical diagnosis is welcome. Colour Doppler study is a simple, reproducible and easily available investigation in most centres.
Methods: We undertook to do Doppler study of intra renal vasculature in non obstructive ARF and to analyze the usefulness in diagnosis and prognosis of ARF.
1. Consecutive cases of non obstructive ARFs were included.
2.Clinical classification of ARF into glomerular disease(AGN) and tubulointerstitial disease(TI) was made using the clinical setting, quantity of proteinuria, type of urinary sediments, ASO, C3 level and renal biopsy wherever available.
3. Cases which could not be clearly categorized into AGN or TI were excluded.
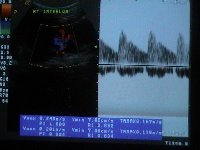
4. Doppler estimation of Resistive Index (RI) and Pulsatile Index (PI) in the interlobar branches of both renal arteries were done. The results were analyzed statistically to see if the indices correlated with the type of underlying lesion and the severity of renal failure.
Results: Total - 83 ; AGN - 43 ; TI - 40
| | RI Mean | PI Mean | Creat Mean |
| AGN | 0.675 | 1.131 | 4.1 |
| TI | 0.753 | 1.454 | 4.9 |
| p | p< 0.05 | p< 0.05 | p> 0.1 |
| | AGN | TI | p value |
| RI > 0.8 | 0 | 22 | <0.01 |
| RI > 0.75 | 5 | 27 | <0.01 |
| RI < 0.7 | 31 | 14 | <0.05 |
Conclusions:
1. In ARF, RI and PI of interlobar artery is significantly higher in Tubulo interstitial than Glomerular disease.
2. There is a positive correlation between RI/PI and severity of renal failure in ARF due to tubulo interstitial lesion and not glomerular lesion.
3. Attention to this variable expression of renal doppler might throw more light into research of the pathophysiology of ARF due to different lesions.
3. Doppler study is a useful tool in evaluation and management of ARF.