|
|
preliminary report
Authors: Kolodziej Waldemar, Latka Dariusz, Krzeszowiec Tomasz, Podgorski Dariusz, Czerwinski Krzysztof Institution: Department of Neurosurgery, State Medical Center, Opole, Poland Email: wkolodziej@wcm.opole.pl Abstract Introduction Cases Discussion Conclussion The authors present two cases of multifocal malignant glioma (one of them simultaneously developed). The tumours were localized supratentorially on both hemisphere of the cerebrum. They were operated in two stages. Histological examinations revealed malignant glioma.in both cases. The outcome was good. The authors discuss this problem and probable mechanism of developing such findings. Review of a literature concernig this problem is also included. Introduction Multifocal gliomas of the central nervous system are rather rarely and uncommon findings. The reported incidence by Shimura is about 2-10% 9 and by Barnard ca. 16% 8 of gliomas (9,5 % was multicentric and 2,9 % had various histological examination results). Mostly they are located supratentorially, very unusually they occur below the tentorium. There is an inconsistently way to name these kinds of glia abnormalities. From Salvati 4 multifocal gliomas are divided to: diffuse, multiple, multicentric and multiple-organ. Whereas mostly you can meet only two main terms: multifocal and multicentric gliomas in the literature. The main features of multicentric gliomas are absence of macroscopic or microscopic connections themselves or way of disseminations (absence of seeding along easily accessible routes). Histological examination often revealed different findings. They should be located in different parts of the brain. Mutlifocal glioma are rather malignant. Usually histological examination revealed the same. They can spread through subarachnoidal space into CSF or blood 4, 12. Multicentric gliomas have independent developing, multifocal are more malignant and develop simultaneously.10 Cause of multifocal localisation they can be mistaken for metastasis 12,13. Cases 53-years old, female, H.D., was admitted after CT-scan which revealed heterogeneous tumour in temporo-parietal region on the left side (5x4x3 cm), contrast-enhancing with oedema and another one in frontal right lobe, hyperdensive, enhancing with contrast. (Figure 1) For two months before admission patient was suffering from reading difficulties and fresh memory disorders. Three weeks later headache appeared, patient became mentally changed. That was the reason to make a CT. On admission patient was conscious, disorientated, GCS 14 pts., with sensory aphasia, fresh memory disorders, no other focal signs. The operation was performed: tumour in temporo-parietal region was resected totally. After the operation mixed aphasia and mild right hemiparesis were observed. During the hospitalisation hemiparesis was abating. During the second operation tumour of the right frontal lobe was resected totally, too. After surgery patient was deteriorate, with very poor contact. CT-scan revealed mass-effect by focus after resected tumour with shift from left side to right. (Figures 2,3) External drainage was performed. Patient got better, was conscious, with mixed aphasia and no focal signs. Because of profusion drainage it has been decided to make a shunt between cavity after tumour resection and peritoneum. Patient was discharged from our Department alert, with mixed aphasia and no other focal signs. Histological examinations both of tumours were Glioblastoma multiforme. Radiotherapy was undertaken. Figure 1 
Figure 2 Figure 3
41-years old, female, A.K., was admitted on account of headache and vertigo (for two weeks before admission) and increasing right hemiparesis and aphasia (last days before admission). CT-scan revealed cystic tumour in the left occipito-parietal region with oedema around, infiltrating and translocating of the callosal. (Figure 4) On admission patient was conscious, GCS 15 pts, right hemianopsia and very mild right hemiparesis were observed. During the operation tumour was resected subtotally because it infitrates the callosal. (Figure 5) Histological examination revealed Glioblastoma multiforme. HistologicalHNeurological signs retreated. Follow-up CT-scan revealed hematoma in a tumour resection’s cavity. Patent did not agree to be operated, then she was treated non-surgically. Follow-up CT showed completely resolution of a haematoma. Outcome was very good. The month after, during radiotherapy, right half of the face numbness and mild right sided hemiparesis were observed.. CT-scan revealed another focal tumour in the fronto-temporal region of a cerebrum. (Figure 6) Patient was operated and a tumour was resected totally. (Figure 7) Histological examinations revealed Glioblastoma multiforme. Outcome was very good, radiotherapy was undertaken again. Figure 4 
Figure 5 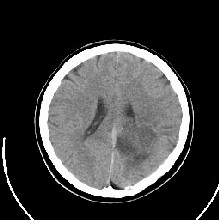
Figure 6 Figure 7 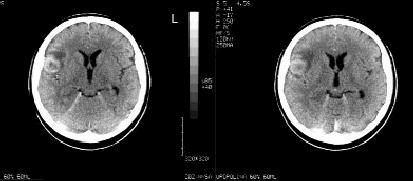 
Discussion We have treated two patients (women) with multifocal malignant glioma. In a case of H.D. there were synchronous lesions, in a case of A.K. metachronous (time interval between tumours was one month). Tumours were resected totally except first one in A.K. In both cases the histological examination revealed Glioblastoma multiforme. As pathological differentiation of the multifocal or multicentric nature of the glioblastoma can be made only at autopsy 11, we can say they were multifocal gliomas on the authority of histological examination. Only H.D. was discharged from hospital with neurological signs as mixed aphasia. Patient A.K. had a full recovery. In both cases sequent radiotherapy was undertaken. Material of 51 cases was described by Kyritsis: 50 % were synchronous and 50% were metachronous; in 14 cases no apparent dissemination route was identified and they were classified into multicenteric gliomas. In the rest of cases, various patterns of spread from a primary site were evident or suggested, these tumours were classified as multifocal 3. It has been also reported material of 21 multifocal malignant gliomas. 11 were developed synchronous, 10 were metachronous (interval of months and years). These kind of mass lesions should be considered in a case with multiple parenchymal masses and no known primary tumour elswhere 7. There is a case of anaplastic astrocytoma with oligodendrogliomatous component found within a vermis and hemispheres of the cerebellum. Later tumour was found within the brain stem and brain hemispheres. Authors suggests that multifocal lesions should be found as multiple metastases from the primary cerebellar astrocytoma via cerebrospinal fluid 1. Very uncommon is evidence of gliomas in one hemisphere. There is a case of coincidence of neurofibromatosis type I and multifocal glioma in frontal and parietal lobe within one hemisphere 5. Angiographic examination revealed both of the tumours with poor vascularisation. One of them in frontal lobe histologically occured astrocytoma pilocyticum, one from the parietal lobe occured low grade glioma. In the author’s opinion gliomas have own natural growing and after that they can get a diffuse form of growing. Shimura described an autopsy case of three tumours: one in the left temporal lobe, one in left parietal one and right fronto-parietal one. Histological examination revealed Glioblastoma multiforme. Autopsy confirmed the CT scan findings and revealed extension of the tumour in the left parietal lobe to the subarachnoid space. By author the main patophysiological mechanisms invoked this are simultaneous neoplastic transformation and seeding from one tumour. Another case report considered evidence of two tumours in a right parietal lobe and one in the left frontal lobe. Biopsy was performed. Histologically were found Oligodendroglioma 6. Very rarely is giant cell glioblastoma, particularly within the cerebellum. From Parekh 2 a month after excision of that tumour, another one was found in the left temporal lobe. Histologically findings were analogical. Another very rare finding is synchronously evidence of supra- and infratentorially glioma.It has been reported two simultaneously developed tumours in both the cerebrum and the cerebellum. Another one occured after two months in the basal ganglia 13. Conclussion Multiple malignant gliomas (multifocal or multicentric) are the rare findings. Pathogenesis is proposed to be multiple malignant induction or spreading from one tumour focus through subarachnoidal space and through cerebrospinal fluid pathways or blood. In a case when a diagnosis of multiple brain tumors is established based on CT examination or MRI, it is recommended to perform biopsy to not to mistake multicentric gliomas as brain metastases. References
|
To contact
Authors personally: wkolodziej@wcm.opole.pl |
|

