|
|
The contralateral trigeminal neuralgia in the course of cerebellopontine angle cholesteatoma.
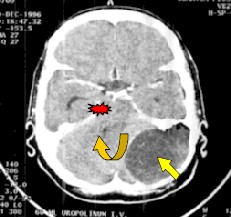
Authors: Krzeszowiec Tomasz, Latka Dariusz, Podgorski Dariusz, Czerwinski Krzysztof, Mrowka Ryszard* * Chair and Department of Neurosurgery, Silesian Medical Academy Bytom, Poland Institution: Department of Neurosurgery, State Medical Centre Opole, Poland Email: tkrzeszowiec@wcm.opole.pl Abstract Introduction Case Report Discussion We report the case of 58 years old woman with giant tumor localised in the left cerebellopontine angle treated surgically. The main symptom was the contralateral trigeminalgia. There are few reports of contralateral trigeminalgia due to tumor localised in the posterior fossa. Basing on the literature the possible mechanism leading to contralateral trigeminalgia is discussed. Change in placement of the brainsteam and compression of contralteral V nerve root is regarded as the cause. Introduction People suffered from trigeminalgia for centuries, the facial pain is also known as ‘tic doloreux’, because of the characteristic face features. The patient experiences pain, usually severe, that occurs suddenly and lasts few seconds to minutes. Pain is described as lancinating or electrical, after attack persist constant discomfort in one side of the face. The pathophysiology of trigeminal neuralgia still needs precise explanation. According to literature the aproximately 90% of trigeminalgias result from mechanical compression of the nerve root by surrounding vessels. Tumor of CPA were causing the face pain in 5-8 % cases. Sclerosis multiplex is the seldom reason /2%/. Contralateral trigeminal neuralgia in posterior fossa tumor is extremely rare. We present our case and compare with literature. Case Report This 58 year-old woman was admitted to the hospital in January 1997. She suffered from intensify pain of head with 6-year history and right sided trigeminal neuraliga of 9 months duration. The nausea appeared in last time. The treatment with carbamazepine was unsuccesful. The neurological examination on admittion was normal. X-ray film revealed osteolisys of the left occipital and temporal bone. The CT scans showed a giant /7x5x4cm/ low density tumor in left posterior fossa, the left cerebellum hemisphere and fourth ventricle was shift to the right ( Figure 1, Figure 2 ). The patient underwent surgery via a left suboccipital craniectomy with total excision of a cystic, pearly tumor – the pathological examination identified: Cholesteatoma. The postoperaitive course was good. At postoperative follow-up: the trigeminalgia progressively dissapeared , she was with the alcoholisation of gasserian ganglion and takes carbamazepine in low doses. The patient returned to her earlier work and feel good. In 1998 control CT scan revealed an empty, aereal place in the operation site (Figure 3).
Figure 3 Postoperative CT, permanent aereal place in operation site. 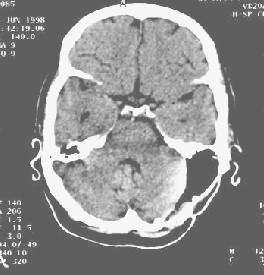
Discusion The etiology of trgeminal nerve dysfunction have been explained from numerous observations made during microsurgical operations for nerve dysfunction syndromes. Trigeminal neuralgia results from cross-compression or distortion of trigeminal root entry zone by elongated loop of vessels. The SCA and AICA are the most frequently found /4/. Tumors also were reported as a cause of ipsilateral neuralgia. There are direct contact, stretchening of the nerve and also artery compression observed at operations /1/. Most frequently there are meningiomas, acoustic neurinomas and epidermoids. The contralateral trigeminalgia due to tumor of posterior fossa are rare. Pathophysiology of these cases are controversial and wait for verify. There is displacement of brainstem in most cases described in articles /2,3,5,6/. There is general agreement, that it is important cause of contralateral nerve dysfunction. The trigeminal sensory root may be compressed between the brain stem and temporal bone or edge of tentorium. Distortion of the brainstem make the sharp angulation entry of Vth n. at Meckels’ cave. Another hipothesis suggests: the CPA tumors make rotation the ventral surface of brainstem to tumor and the anteriorly directed trigeminal nerve stretched at its dural foramen /5/, so the size and nature of the tumor have a role in the pathogenesis On the other hand an alternate explanation for this symptom is presence of a cross-compession by contralateral vascular structure – the BA or SCA may be displaced by the mass and formed an ‘arterial loop’ in conflict with trigeminal nerve root /3/, that hypothesis agrees with typical etiology of trigeminalgia. At last an arachnoid strongly adhesions and disturbances of CSF flow played the role in pathogenesis of trigeminal dysfunction /5/. Table 1Factors in contralateral trigeminalgia /5/.
Optimum strategy for the treatment of contralateral trigeminal neuralgia is to remove the reason /tumor/ and allow the structures of posterior fossa to return to its normal position and relief patient of the pain. When the postoperative course is unfovurable and the symptom still persists, the exploratory microsurgical decompression of contralateral trigeminal nerve may be concerned. References |
To contact
Authors personally: tkrzeszowiec@wcm.opole.pl |
|